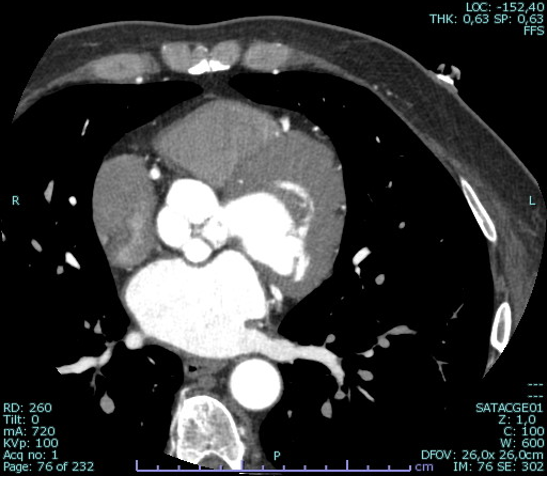
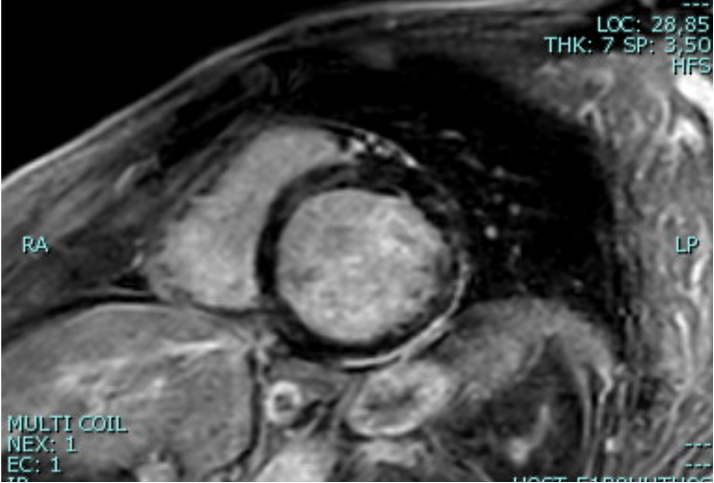
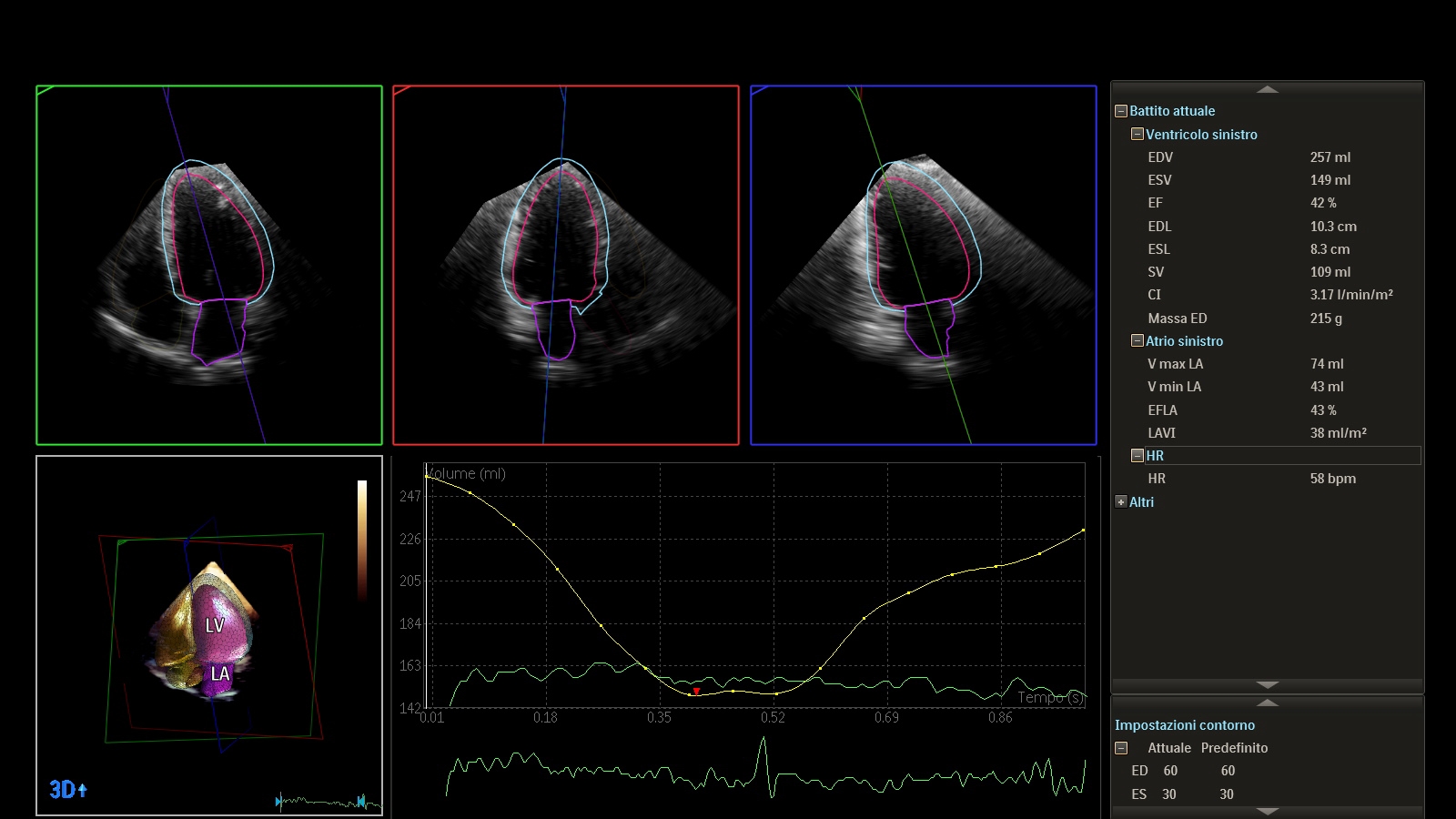
Muscular dystrophies of the limbs are a group of heritable genetic disorders that mainly affect the pelvic or shoulder girdle muscles, causing progressive weakness. Although the underlying genetic origin varies widely, a cardiac involvement has been frequently observed in neuromuscular disorders. Therefore, cardiac imaging is an indispensable part of surveillance and management of muscular disorders. This is the case of a 48 years old man with a recent diagnosis of limb-grindle muscular dystrophy. Initial genetic testing uncovered a variant of uncertain significance in heterozygosis in the MYH7 (myosin heavy chain 7) and SYNE 1 (synaptic nuclear envelope protein 1) genes, negative for dystrophin gene mutation. As part of the diagnostic workup, an echocardiogram, performed despite the absence of specific symptoms and cardiovascular risk factors, revealed the presence of dilated cardiomyopathy with reduction of ejection fraction. To rule out coronary involvement, a coronary CT scan was performed with the curious finding of quadricuspid aortic valve (type II, Nakamura’s classification system) and anomalous origin of the left coronary artery from the non-coronary sinus with benign course in the absence of hemodynamically significant stenosis (Figure 1). Given the prognostic value associated with tissue characterization, the patient also underwent cardiac magnetic resonance with evidence of extensive late gadolinium enhancement with a non-ischemic pattern involving the inferior basal segments, the infero-septal mid-ventricular segments, and the apical segments of the anterior and lateral walls (Figure 2). In view of the cardiological findings, optimized heart failure therapy based on the four pillars ( angiotensin receptor-neprilysin inhibitors after a period of angiotensin-converting enzyme inhibitors, sodium-glucose co-transporter 2 inhibitors, mineralocorticoid receptor antagonist , beta-blockers) was introduced. The follow-up echocardiogram at three months showed initial reverse remodeling with partial recovery of ejection fraction (Figure 3). Therefore, genetic testing has been undertaken to rule out mutations in genes associated with a high risk of sudden cardiac death ( desmoplakin, filamin C, lamin A/C, phospholamban, RNA binding motif protein 20 ), in accordance with ESC guidelines. Results are not yet available. Given the complex pathophysiology of these disorders, patient management remains a challenge for clinical cardiologists.