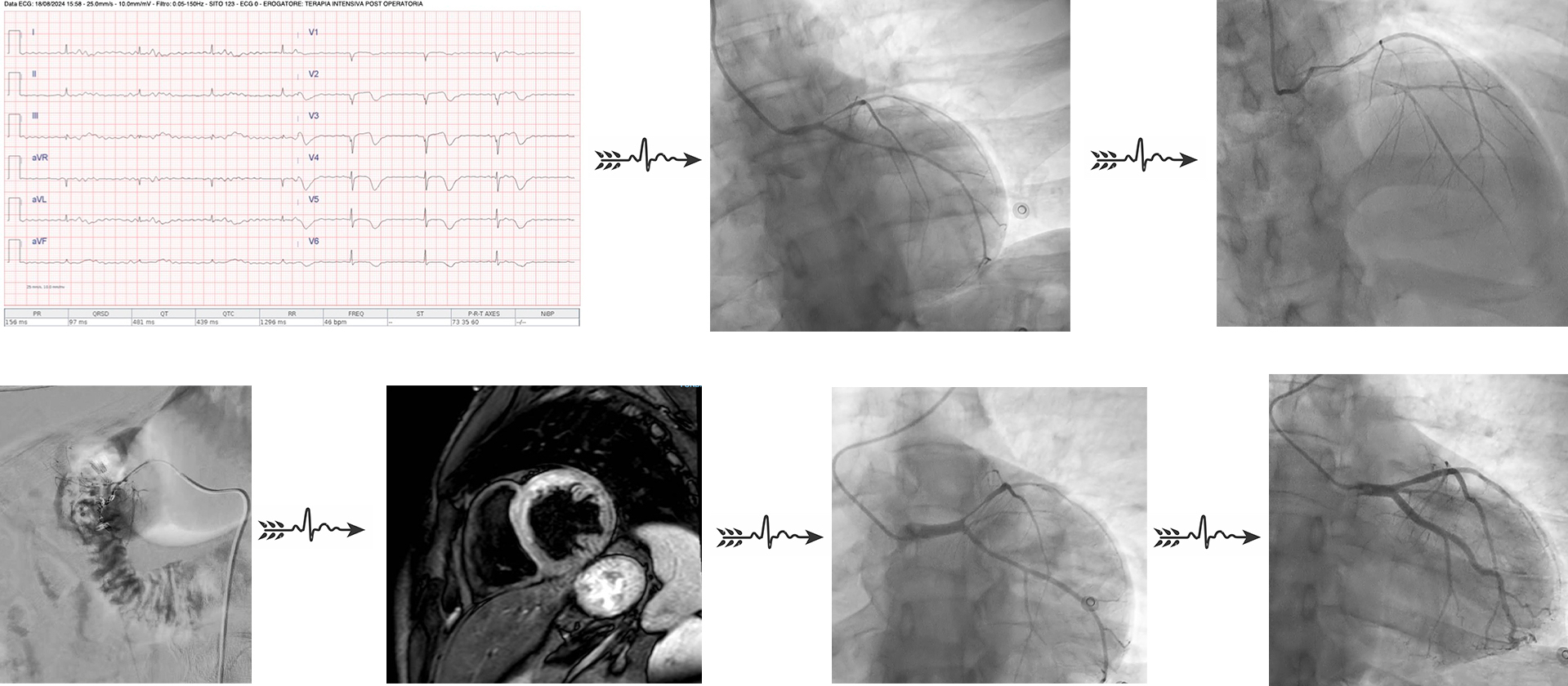
Rationale A patient with a history of alcohol abuse presented to the emergency room with band-like abdominal pain, melena, and severe acute anemia. After blood transfusion and urgent esophagogastroduodenoscopy revealing multiple duodenal hemorrhages (treated with adrenaline hemostasis), the patient was transferred to the intensive care unit (ICU). In the ICU, a marked troponin elevation (40,000 ng/L) was observed alongside ST-segment elevation on the ECG. Urgent coronary angiography showed severe diffuse vasoconstriction in all three coronary vessels, likely due to hemorrhagic shock and norepinephrine infusion. Atherosclerotic plaques were noted in the mid RCA, proximal LCx, and proximal LAD but were not deemed quantifiable. Revascularization was postponed due to systemic instability. The patient then experienced two episodes of ventricular fibrillation, both successfully treated with DC shocks. An abdominal CT scan subsequently revealed active endoluminal bleeding in the superior duodenum: an angiographic embolization of the gastroduodenal artery stabilized the patient’s hemodynamics. Technical Resolution The case was discussed in a Heart Team session due to its complexity. Cardiac MRI and a second coronary angiography were performed. The MRI showed moderate left ventricular dysfunction and subacute infarction in the LAD territory. The second angiography identified an intermediate stenosis in the proximal LAD, deemed non-functionally significant (FFR 0.84). Additionally, a vasospasm in the proximal LAD was observed and resolved with intracoronary nitrates, leading to a diagnosis of vasospastic angina. The patient was considered for treatment with diltiazem, pending improvement in ventricular function. Clinical Implications This case underscores the importance of multidisciplinary management in acute cardiac conditions. Initially presenting with cardiogenic shock due to anemia from gastric bleeding linked to alcohol abuse, the patient underwent multiple stabilizing procedures, including esophagogastroduodenoscopy, coronary angiography, cardiopulmonary resuscitation, and arterial embolization. While a straightforward diagnosis of type 2 myocardial infarction due to anemia could have been sufficient, the Heart Team’s decision to conduct additional imaging uncovered vasospastic angina as a contributing factor. This comprehensive approach allowed for tailored therapy to address the underlying condition and reduce the risk of future angina episodes.