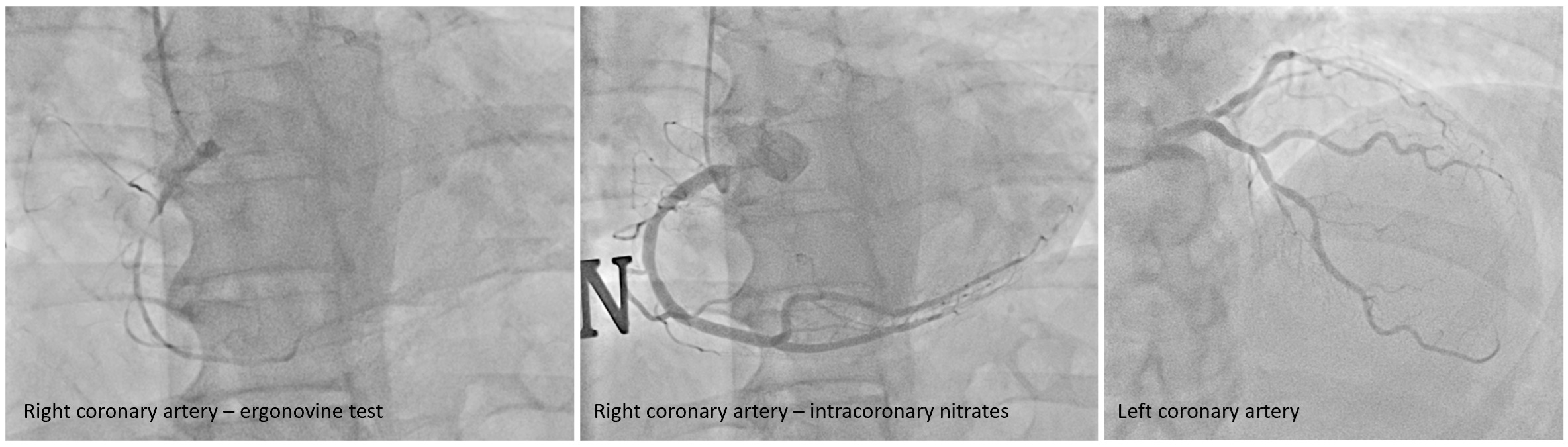
Background: ST-segment elevation is typically associated with acute coronary syndromes; however, it can also mask less common conditions, such as coronary vasospasm. Ischemia caused by coronary vasospasm can not only mimic myocardial infarction but also lead to conduction abnormalities, including atrioventricular block.This case highlights the diagnostic challenges posed by transient ST-segment elevation and AV block, emphasizing the need to consider vasospasm as a potential underlying cause. Case Presentation: A 58-year-old female with no significant history presented to our department with chest pain and syncope. Initial non-invasive investigations were unremarkable and coronary angiography revealed diffuse atherosclerosis with critical stenosis in the anterior interventricular coronary artery. The patient underwent successful percutaneous coronary intervention with a biolimus-eluting stent and dual antiplatelet therapy was started (Fig.1). After coronary revascularization, the patient again experienced symptoms characterized by chest pain and arm tingling. Telemetry showed transient ST-segment elevation of 4 mV, accompanied by bradycardia and Type II atrioventricular block (BAV) grade I and 2:1 without significant pauses were noted (Fig.2). A second coronary angiography with an ergonovine test was performed and revealed severe spasm of the right coronary artery with near-total occlusion, which triggered the recurrence of symptoms and ST elevation on the ECG. The vasospasm and the resulting symptoms were resolved with the administration of intracoronary nitrates (Fig.3). The patient was subsequently treated with diltiazem and long-acting nitrates, and at the 30-day follow-up, she remained completely symptom-free. Discussion: This case highlights the challenges of diagnosing chest pain with transient ST-segment elevation, where coronary vasospasm and atherosclerosis coexist. These conditions can mimic acute coronary syndromes, leading to potential misdiagnoses. Dynamic ECG changes and conduction abnormalities, such as AV block, further complicate the clinical presentation. Prompt recognition of vasospasm is crucial, as it requires vasodilators rather than revascularization alone. A comprehensive diagnostic approach, including telemetry, coronary angiography, and provocative testing, is essential for accurate diagnosis and effective management.