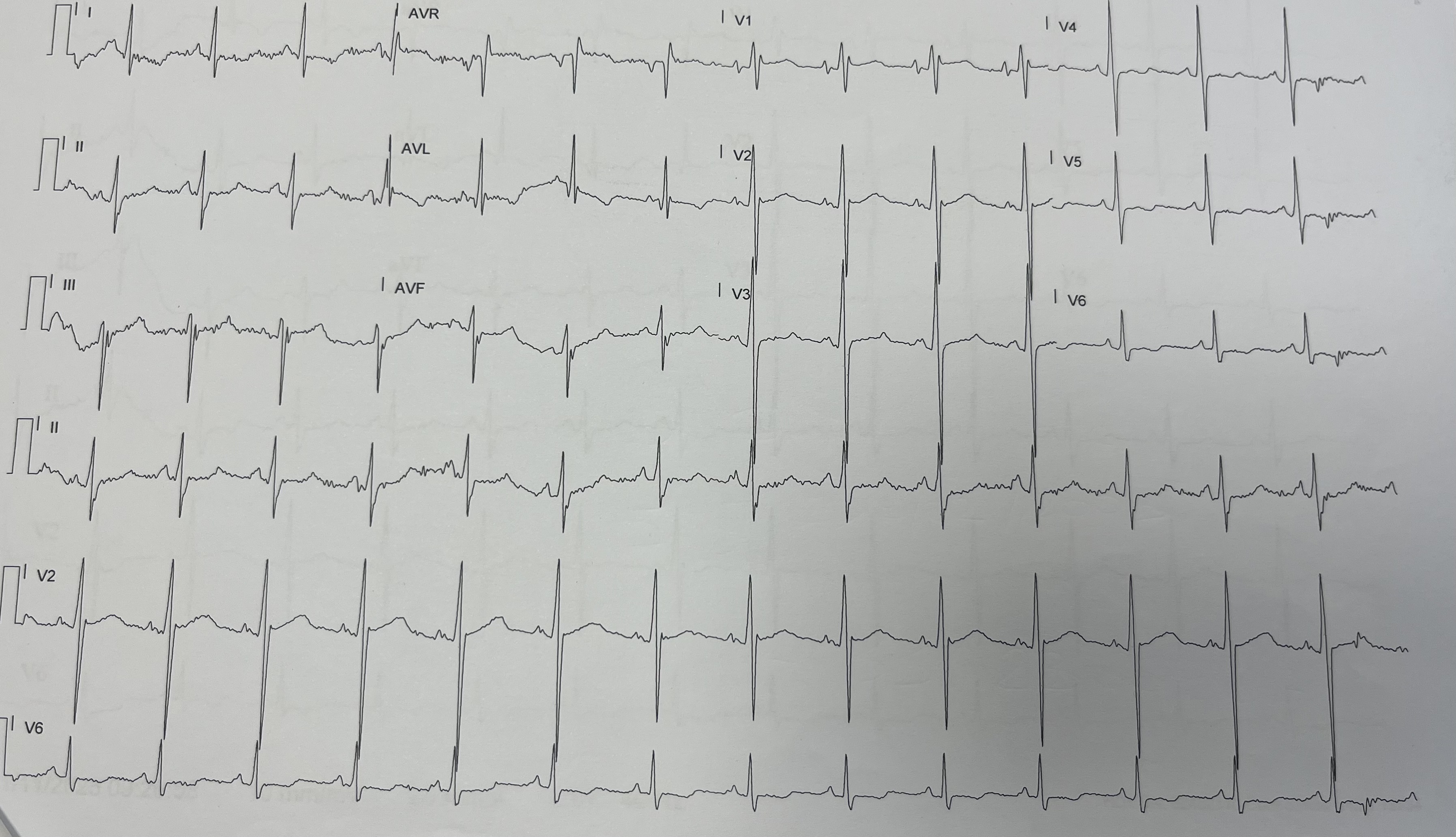
Background Hypertrophic cardiomyopathy (HCM) is a genetically determined myocardial disorder defined by unexplained left ventricular hypertrophy. Although frequently asymptomatic in the early stages, it remains one of the leading causes of sudden cardiac death in young individuals and athletes. Detecting subtle manifestations of the disease during routine screening plays a pivotal role in preventing adverse outcomes and guiding clinical decisions. Case Presentation A 24-year-old competitive male athlete with no known cardiac history underwent a routine sports eligibility evaluation. Despite excellent physical conditioning and complete absence of cardiologic symptoms, his resting electrocardiogram (ECG) revealed unexpected nonspecific repolarization abnormalities. Given his athletic profile, these findings prompted further investigation. Exercise stress testing was performed and completed without chest pain, arrhythmias, or hemodynamic abnormalities. However, due to the suspicious baseline ECG, a transthoracic echocardiogram was obtained. Imaging disclosed disproportionate hypertrophy of the interventricular septum, with preserved systolic function—an unexpected result in an otherwise asymptomatic and highly trained athlete. To refine the diagnostic assessment, cardiac magnetic resonance imaging (CMR) was conducted. CMR not only confirmed septal hypertrophy but also demonstrated mid-wall late gadolinium enhancement (LGE) localized to the septum, indicating the presence of myocardial fibrosis—a finding associated with increased arrhythmic risk in HCM. A 24-hour Holter ECG showed no clinically significant arrhythmias, but genetic testing identified a pathogenic sarcomeric mutation, definitively establishing the diagnosis. Conclusions This case underscores how a seemingly routine sports evaluation may unveil early-stage HCM in a completely asymptomatic athlete. The combination of ECG, echocardiography, CMR, and genetic testing enabled precise characterization of the disease phenotype, including the detection of myocardial fibrosis with potential prognostic implications. Early diagnosis allowed timely risk stratification, individualized guidance regarding competitive athletic activity, and initiation of family cascade screening. This case exemplifies the critical role of a multimodal, multidisciplinary approach in identifying concealed cardiac disease and preventing potentially life-threatening events in young athletes