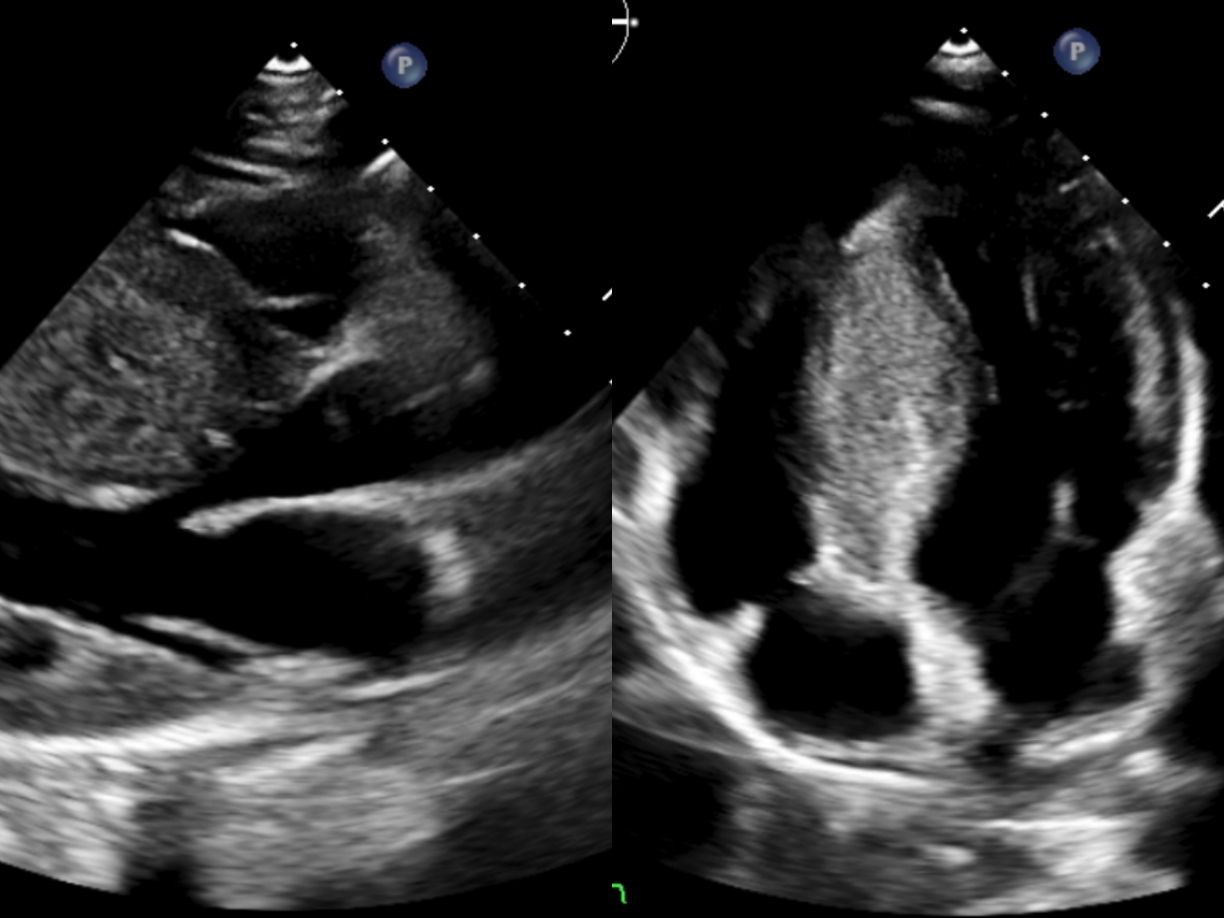
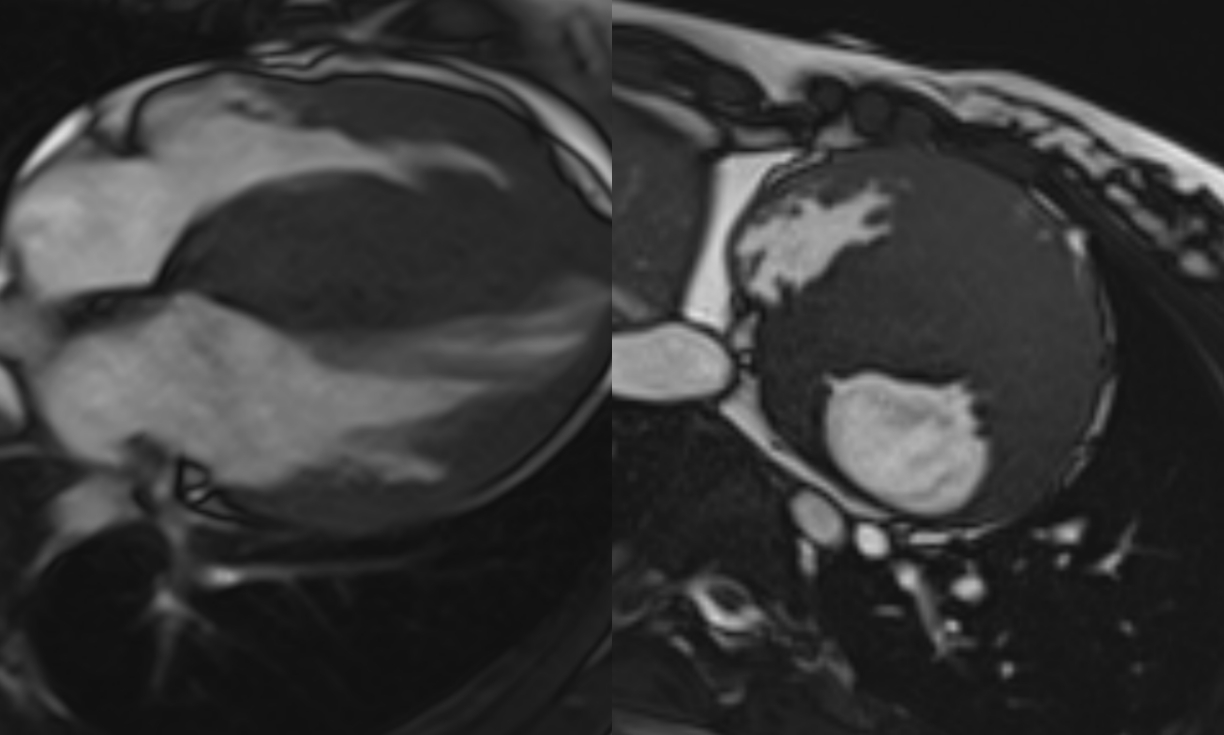
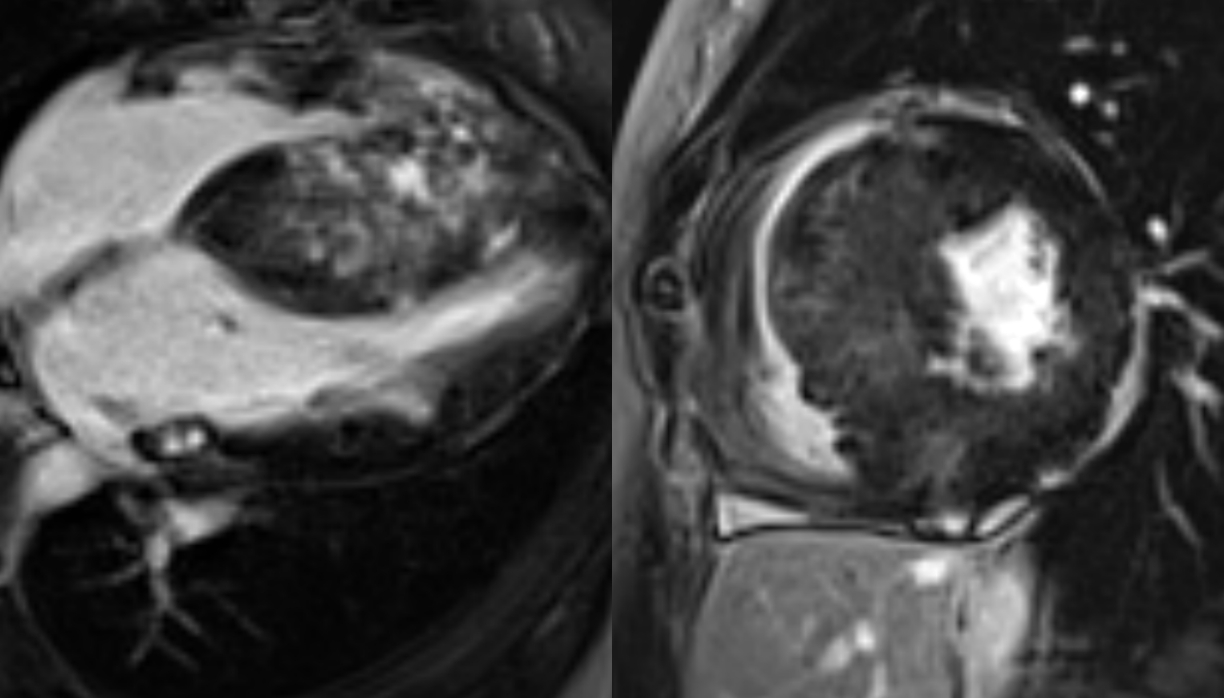
Hypertrophic cardiomyopathy (HCM) is the most common genetic cardiovascular disorder and it has an extremely variable clinical presentation. Here we report the case of a young patient, with no previous cardiac history or cardiovascular risk factors, presenting to the emergency department with chest pain, electrocardiographic changes, and troponin elevation. The diagnosis of hypertrophic cardiomyopathy was immediate following echocardiographic evidence of a massive form of left ventricular septal hypertrophy (44 mm), leading to left ventricular outflow tract obstruction with a dynamic gradient. Characterization of the clinical picture and prognostic risk was further expanded by cardiac magnetic resonance imaging, in particular through tissue characterization, which allowed the identification of diffuse fibrosis through native T1 mapping, edema through T2 mapping, and extensive non-ischemic intramyocardial replacement fibrosis with late gadolinium enhancement. Given the patient’s young age, the extensive fibrosis on magnetic resonance imaging, and the documentation of episodes of non-sustained ventricular tachycardia on telemetry monitoring, the patient underwent implantation of an sICD for primary prevention due to a high risk of sudden cardiac death according to both European and American guidelines. A genetic analysis was also performed, revealing pathogenic mutations in the sarcomeric genes MYBPC3 and TNNT2. Subsequent echocardiographic follow-up showed a progressive reduction of the intraventricular outflow tract gradient thanks to medical therapy with metoprolol and disopyramide, as well as an almost complete resolution of the patient’s symptoms. This clinical case is therefore particularly noteworthy because of the echocardiographic and magnetic resonance presentation and opens the discussion on the role of the latter in the prognostic assessment of the disease.