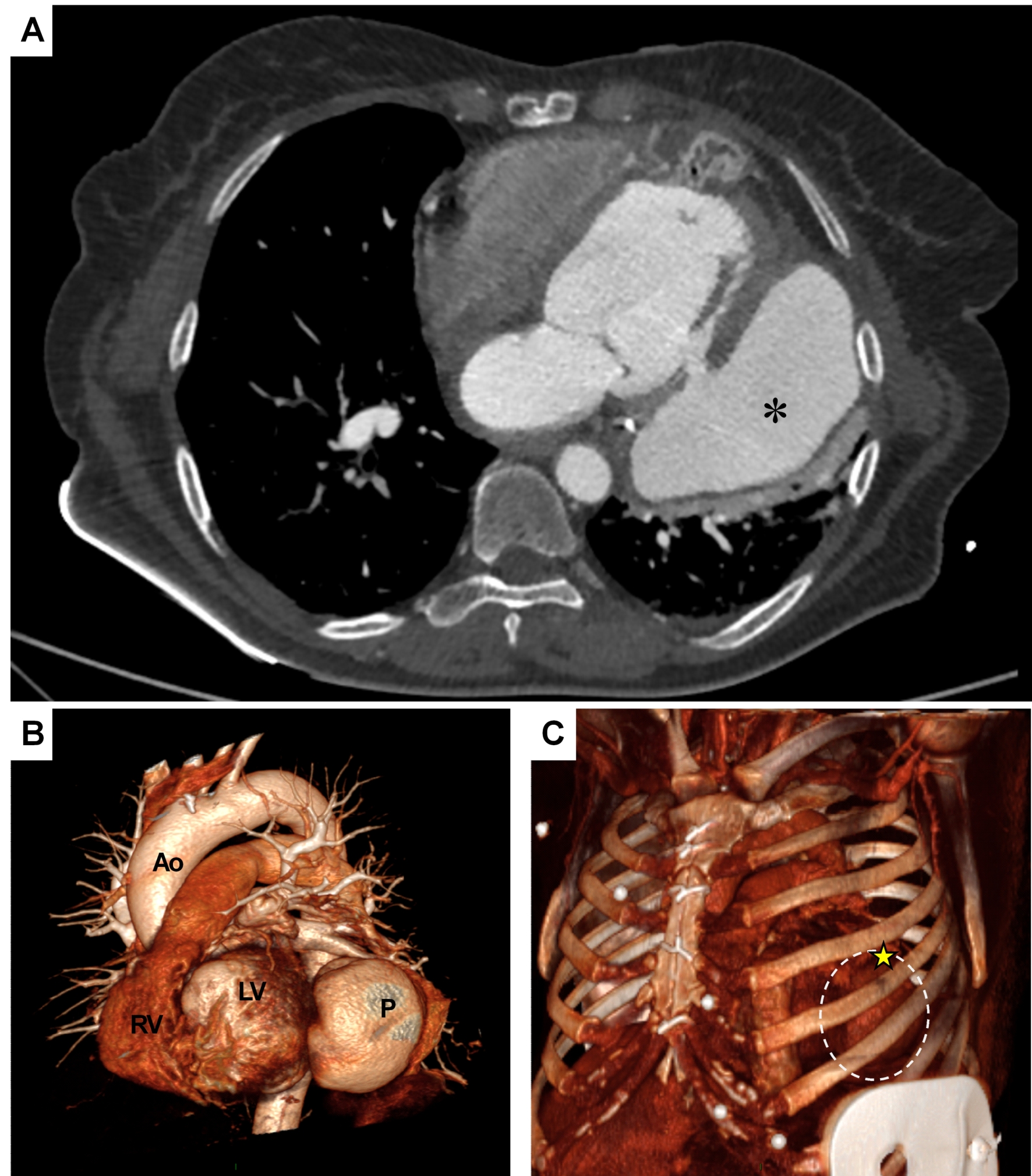
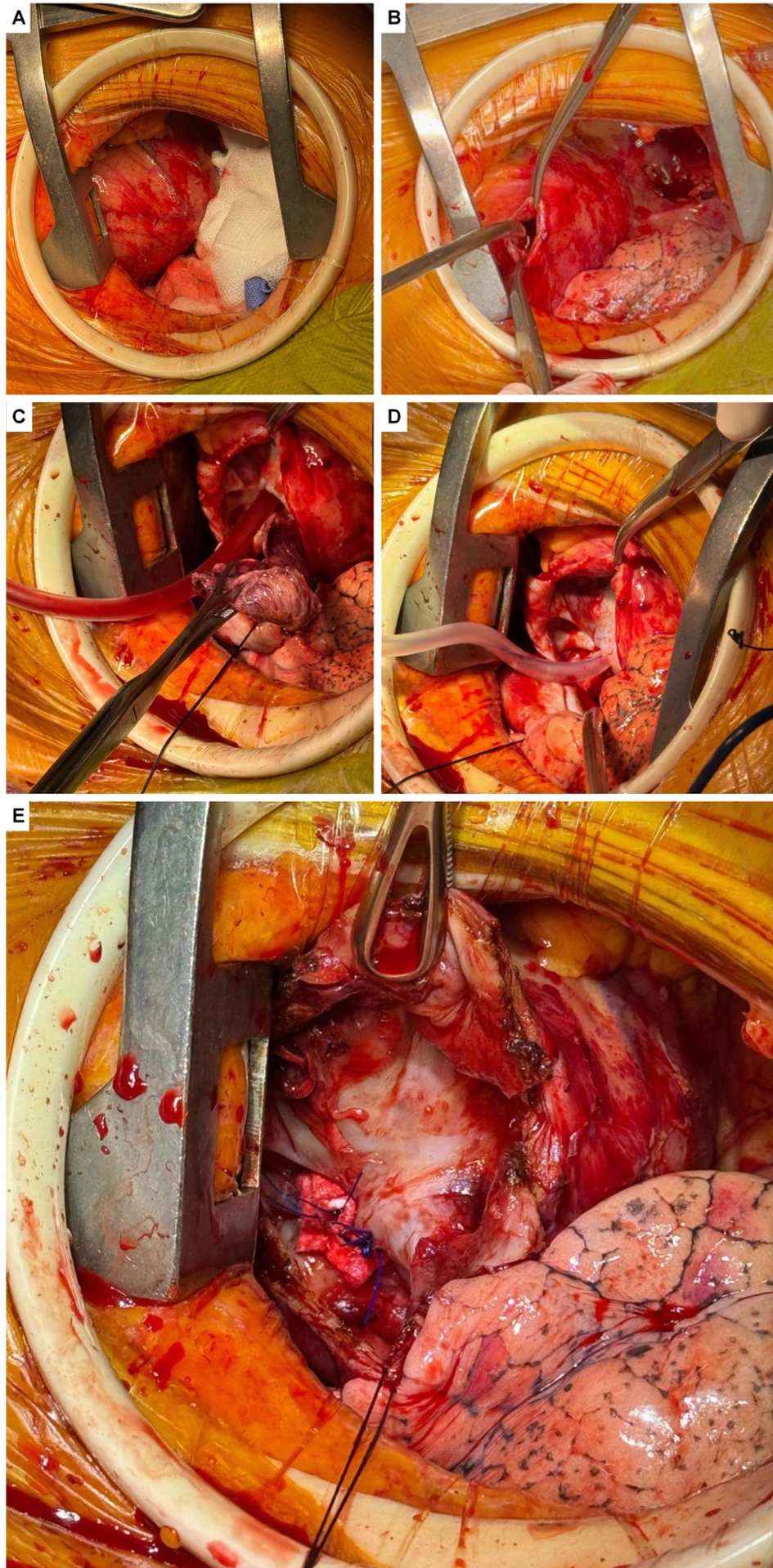
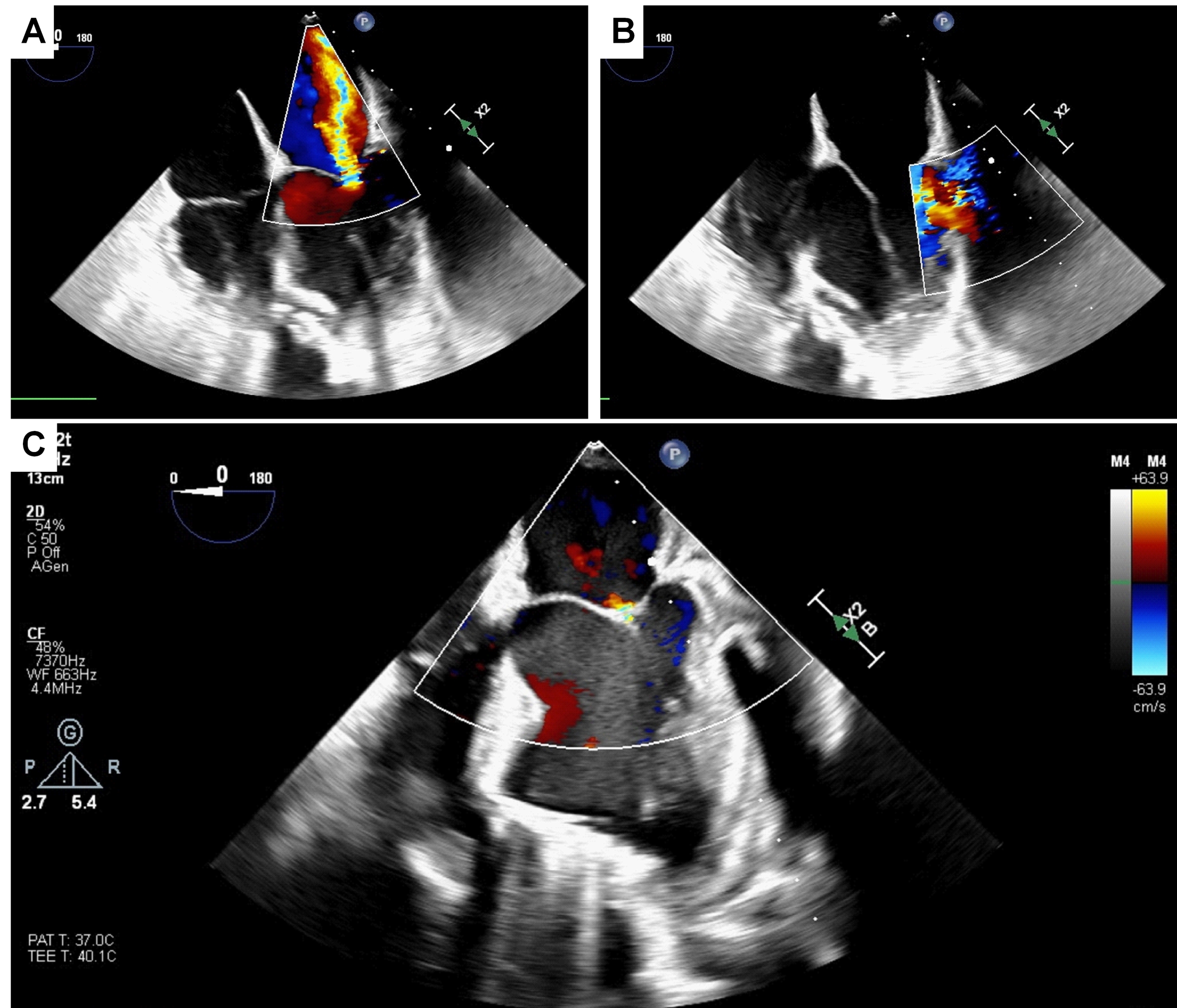
A 66-year-old female presented to the Emergency Department following an incidental finding of a large pseudoaneurysm supplied by the inferoposterior left ventricular (LV) wall during an outpatient echocardiogram. The condition was associated with severe mitral regurgitation (MR) and reduced ventricular function (LVEF 35%). The patient’s history included a subacute anterior myocardial infarction two years prior (in Bulgaria), complicated by an apical-mid ischemic ventricular septal defect (VSD). Coronary angiography at the time revealed occlusion of the LAD. An IABP was placed, and she underwent emergency surgical VSD closure with a patch. Months later, she underwent a second surgery due to VSD recurrence. One year later (in Germany), she was hospitalized for dyspnea and recurrent myocardial infarction; angiography showed circumflex artery disease, which was treated with PCI. The day before the current admission, she underwent outpatient echocardiography due to reported recent syncope and dyspnea on minimal exertion. The echo revealed a thinned posterior LV wall with a 2 cm breach traversed by flow, communicating with an extensive 5 cm pericardial collection. Preoperative workup included coronary angiography, which showed no revascularizable coronary disease. The diagnosis was confirmed via CT angiography ( Figure 1 ). Following a right mini-thoracotomy at the 4th intercostal space and establishment of femoro-femoral cardiopulmonary bypass, the pseudoaneurysm was visualized. Upon opening the external chamber, repair was performed using a circumferential Prolene suture followed by interrupted Prolene U-stitches reinforced with pledgets ( Figure 2 ). This technique allowed for the relocation of the papillary muscles, reducing interpapillary muscle distance and achieving good leaflet coaptation as confirmed by real-time transesophageal echocardiography ( Figure 3 ). The postoperative course was uneventful; the patient was extubated on postoperative day 1 and discharged to a rehabilitation facility the following week. Postoperative echocardiography demonstrated the absence of residual mitral regurgitation due to the modification of ventricular geometry and indirect relocation of the papillary muscles. In conclusion, chronic mechanical complications of myocardial infarction require a multidisciplinary strategy to tailor high-risk, complex interventions to the specific patient profile in order to minimize procedural risks.