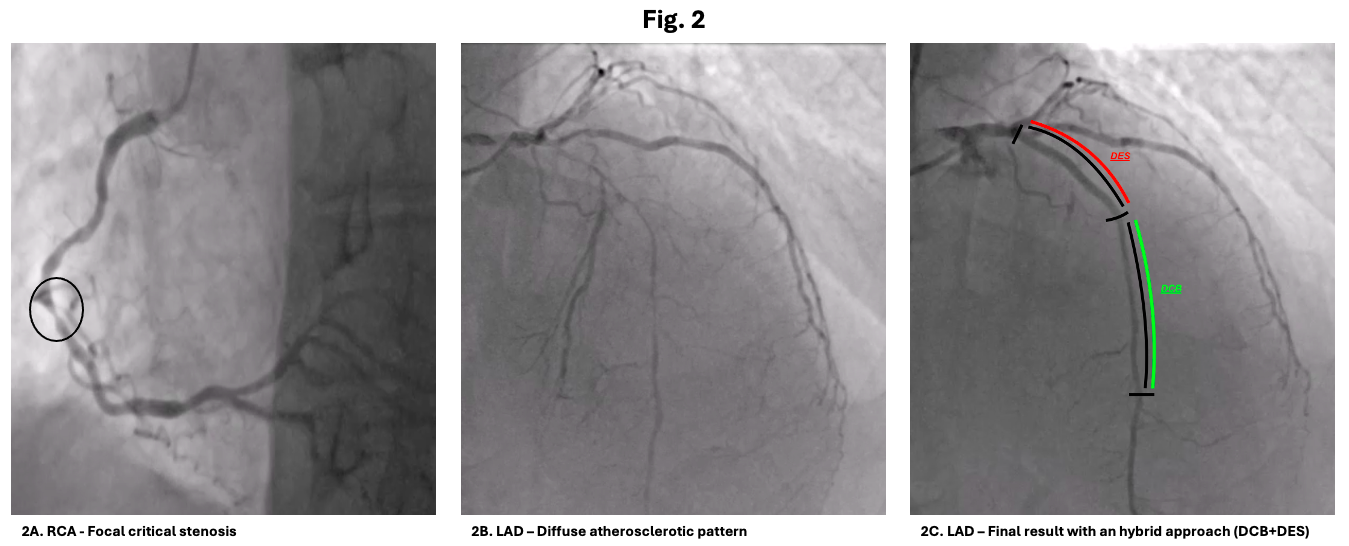
Background: Acute coronary syndrome in patients with hemophilia is a rare but challenging scenario since a double high risk of thrombotic and bleeding complications has to be faced (fig.1). Case report: We present the case of a 64-years-old man admitted to our department for NSTEMI with a mildly reduced left ventricle ejection function (LVEF 48%) due to apical akinesia. The patient had a history of severe hemophilia A (Baseline Factor VIII <3%) and HCV-related cirrhosis. The coronary angiography showed a right coronary artery (RCA) critical stenosis and a long severe left anterior descending artery (LAD) stenosis (fig.2A-2B). Given the complexity of the coronary lesions and the very high hemorrhagic risk related to hemophilia A, the patient was evaluated by the local heart team along with a hemophilia expert. Despite the acceptable peri-operative surgical risk (EuroSCORE II 4% and STS Risk Score 2%), the patient’s frailty was mostly related to the hemophilic status, the comorbidities and the poor family background. So, finally he was elected to percutaneous revascularization with the following endovascular approach for the diffuse severe LAD lesion: the lesion was entirely predilated, using semi-compliant balloon, 1:1 size according to the reference vessel diameter (RVD). We obtained a stent-like result in the mid-distal LAD, whereas on the proximal segment a bad linear dissection occurred. Therefore, the procedure was completed by drug coated balloon (DCB – Magic touch 2,0/25 mm, 2,25/20, 2.5/25 mm) of mid-distal LAD and by stenting of proximal LAD, using a polymer-free drug eluting stent (DES – Biofreedom 3,0/33 mm) suitable for 1-month DAPT (aspirin and clopidogrel) with a good final result (fig.2C). The patient was discharged with the recommendation to continue FVIII concentrates prophylaxis therapy to keep trough levels around >30% during DAPT. Discussion: The current management of patients with ACS and bleeding disorders such as hemophilia is supported only by small retrospective studies or consensus statements. A multidisciplinary team with an expert hematologist is essential to define properly the therapeutic strategy which should balance both the thrombotic and bleeding risks. In patients with a diffuse atherosclerotic pattern, a strategy encompassing DCB alone or in combination with spot stenting could be an attractive alternative to a full-length DES implantation, allowing a short DAPT regimen imposed by the concomitant hemophilia.