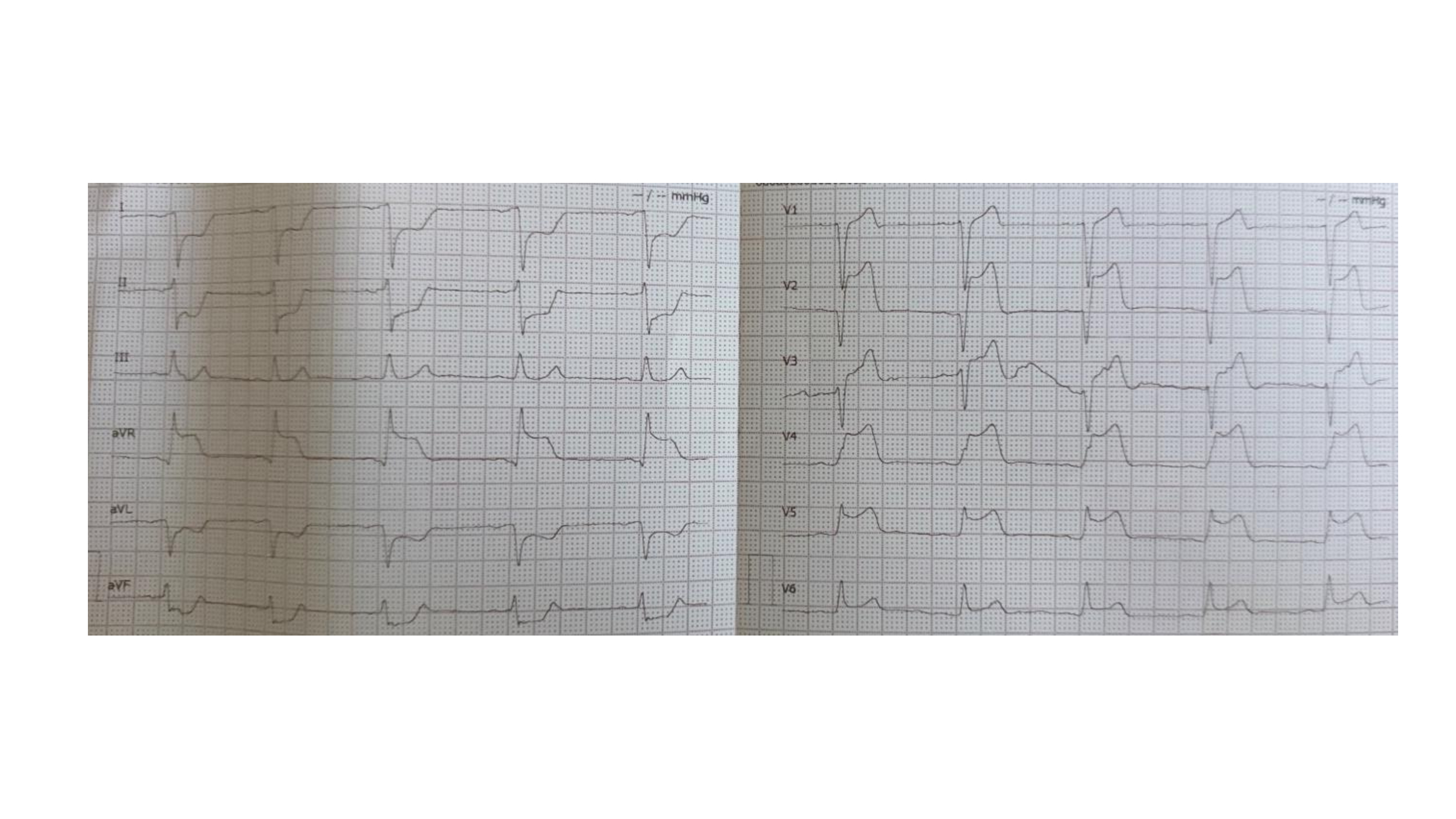
Introduction: SCAD is an important cause of MI and accounts for up to 35% of ACS. While SCAD due to psychiatric disorders has been reported in the literature, SCAD during the management of drug withdrawal has not. Case report: A 47-year-old male was admitted to the ED of “San Giuseppe Moscati” Hospital for chest pain. The ECG revealed ACS-ST-elevation MI. The patient was referred to our cath lab. ICA showed a distal occlusion of the left coronary artery due to SCAD. A BMW Universal II guide was attempted, as recanalization of the vessel was unsuccessful. The echocardiogram showed reduced global left ventricular kinesis (35%). The patient was transferred to the intensive cardiology unit for further management. A history of addiction was noted in the past medical history. The patient had received his last dose of the drug roughly two days prior. Hence, the patient underwent serum dosage of abused substances. The serum levels of benzodiazepines and cannabinoids were high, while the concentration of opiates was at the high limits of normal. Meanwhile, the patient was given methadone to mitigate withdrawal symptoms. Therefore, the patient was discharged with ACS caused by SCAD, HF with reduced ejection fraction, and methadone in the cardiac rehabilitation unit for a forty-day re-evaluation. Discussion: Nevertheless, a differential diagnosis between SCAD and atherosclerotic disease is mandatory to optimize clinical management. Given this clinical picture, the most common patient phenotype associated with SCAD is the most important to avoid misdiagnosis and delays in diagnosis. Clinicians should recognize the mentioned risk factors to raise the pre-test probability of SCAD. Risk factors to consider include gender, age, pregnancy, estrogen-progestogen use, inherited connective and vascular diseases, as well as psychiatric factors. In addition, strenuous exercise may play a mechanical role as a trigger for SCAD in susceptible individuals However, SCAD has not been described during drug withdrawal crisis. The case we present had a 3-day opioid-free interval and low toxicology of opioids in serum. The pathophysiological mechanisms of SCAD during withdrawal, however, are unknown. Conclusion: SCAD is a non-atherosclerotic form of ACS. The diagnosis of SCAD is essential for the correct management of the patient. The diagnosis is based on a multiparametric approach, and among the risk factors, psychiatric factors must be considered, including withdrawal.