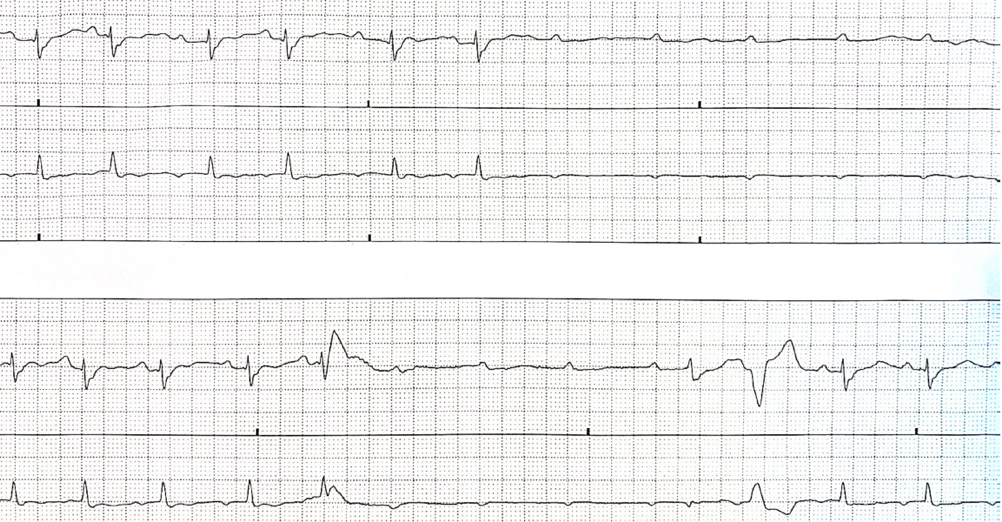
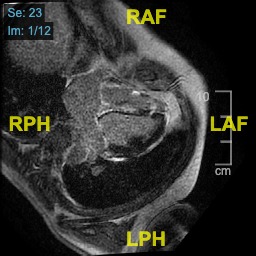
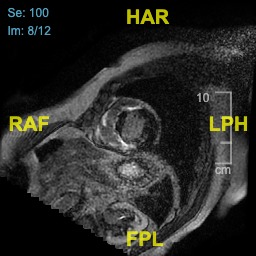
We present the case of a 53-year-old patient without any significant cardiac history. He came to our emergency department following a syncope which was not preceded by prodromes. The electrocardiogram showed sinus rhythm with Q waves in the inferior leads and right bundle branch block. Both HS T troponin and NT proBNP were significantly increased. The echocardiogram showed akinesia of the interventricular septum and of the inferior wall, left ventricular ejection fraction 45%, no valvular pathologies and a normal right ventricle. The Brain CT and the CT-pulmonary angiogram were normal. During continuous electrocardiographic monitoring there were episodes of paroxysmal total atrioventricular block (R-R max 4 sec). The coronary angiography showed healthy coronary arteries. Given the possibility of myocarditis, immunosuppressive therapy with high-dose steroids was started and an endomyocardial biopsy was promptly performed. The diagnosis was acute giant cell myocarditis. The patient was then transferred to a tertiary center where he was treated with high-dose intravenous methylprednisolone, immunoglobulins and cyclosporine, without any need for inotropic or mechanical cardiac support. The cardiac magnetic resonance result was myocarditis with biventricular involvement and a relevant portion of edema and late enhancement, LVEF 35-40%. During hospitalization the patient expressed plateau troponin T HS movement with slow normalization, frequent ectopic ventricular beats and non sustained ventricular tachycardia with stable hemodynamics, which was then reduced with amiodarone. The laboratory showed renal failure with creatinine level of 1.5 mg/dl. Discharged with life vest, he subsequently underwent subcutaneous ICD implantation after an MRI which showed reduction of the inflammatory component and fibrosis with an intramyocardial pattern. During a follow up visit, one year later, the LVEF was 38%. Accurate and early diagnosis with EMB in patients with GCM is crucial for better outcomes. A rapid initiation of methylprednisolone reduces the risk of death. Sustained treatment with a combination of immunosuppressive agents together with optimal heart failure medications is essential for myocardial recovery and long-term stabilization. In our case, the absence of coronary disease and the presence of paroxysmal atrioventricular block even in the absence of haemodynamic instability allowed us to hypothesise the necessity of early biopsy to reach the diagnosis.