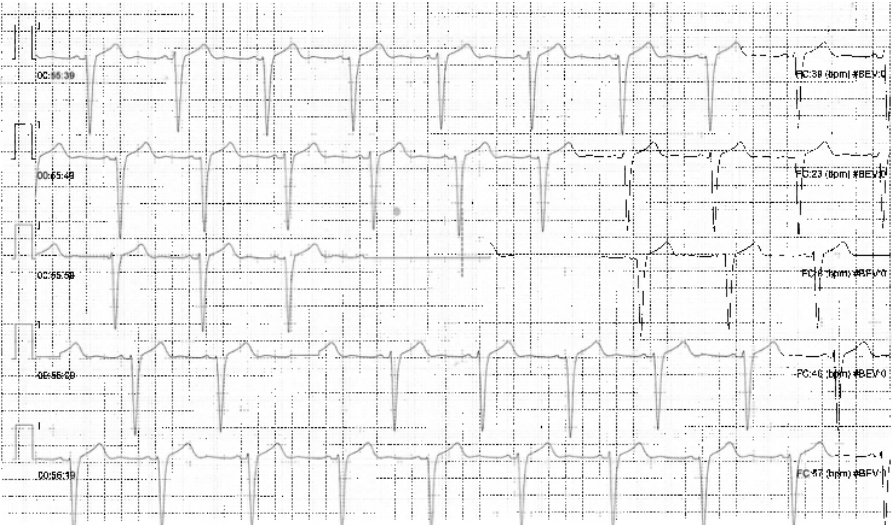
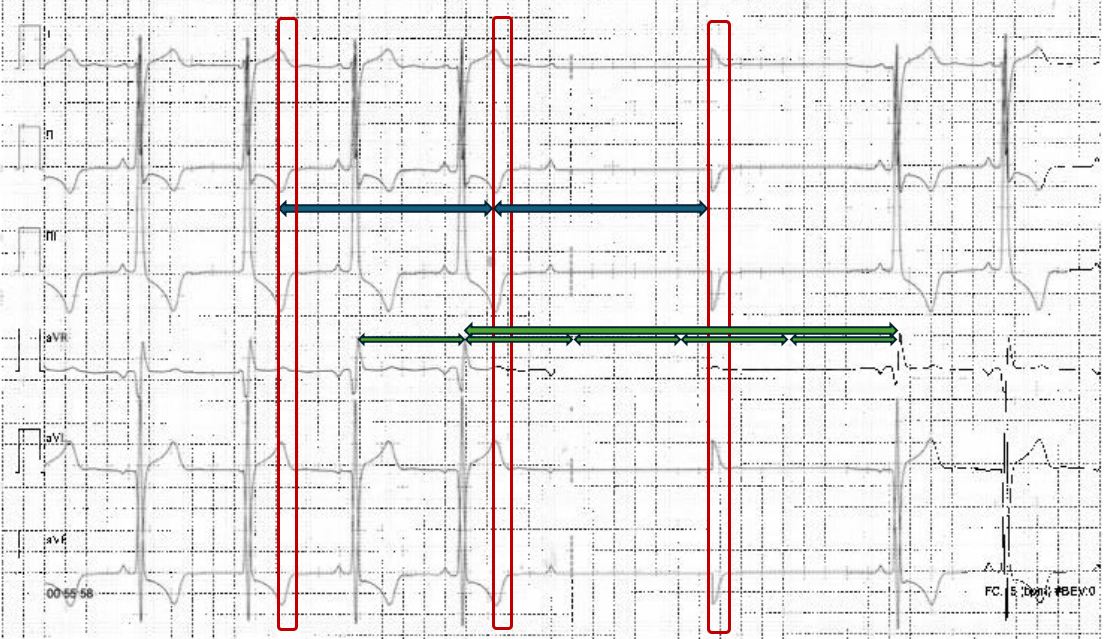
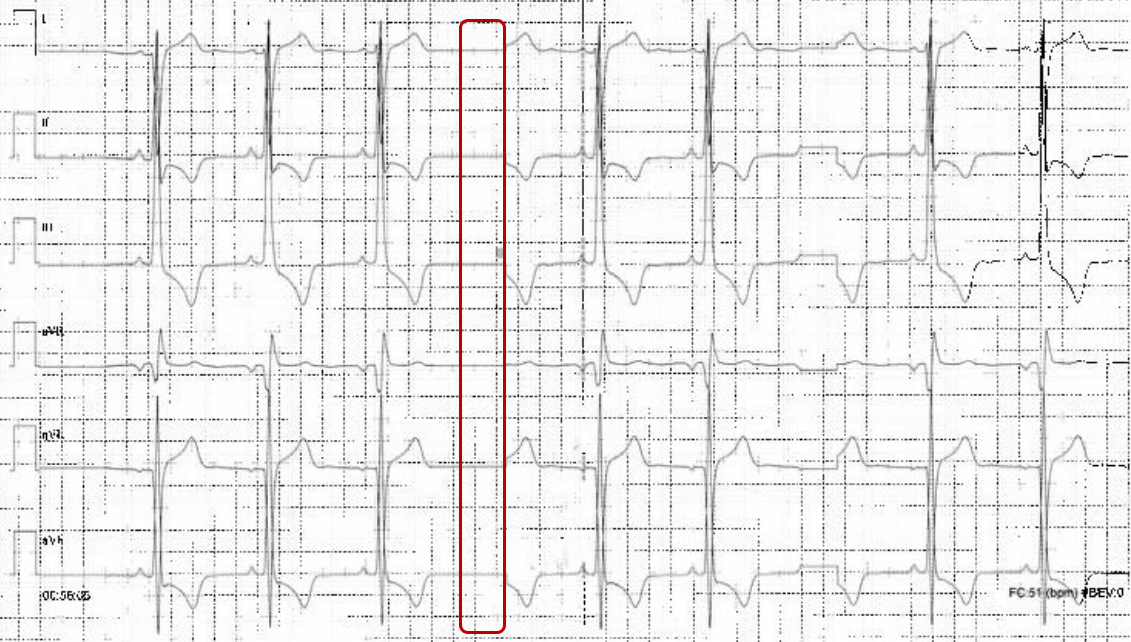
A 72-year-old woman was admitted for evaluation of hypokinetic dilated cardiomyopathy, along with heart failure with reduced ejection fraction (HFrEF). It was incidentally discovered during pre-operative cardiology assessment for carotid endarterectomy, due to critical left internal carotid stenosis. Her history included recurrent presyncopal episodes with prodromal symptoms and absence of palpitations, dyspnea or angina, typically triggered by vagal stimuli such as orthostatism or exertion. Additional comorbidities included anorexia (BMI 16 kg/m²), major depressive disorder, and rheumatoid arthritis. Chronic therapy consisted of acetylsalicylic acid, statins, antidepressants, and immunosuppressive agents. On admission, transthoracic echocardiography (TTE) showed a dilated left ventricle (LV) with an EF of 25% and grade II diastolic dysfunction, without valvulopathy. Other TTE signs were consistent with increased pulmonary resistance. ECG revealed sinus rhythm with newly diagnosed left bundle branch block (LBBB) and T-wave inversion in lateral and inferior leads. Coronary angiography excluded obstructive coronary artery disease. A diagnosis of HFrEF was established, and medical therapy (MT) was initiated and optimized. At discharge, LVEF remained unchanged, while pulmonary resistance normalized. During continuous ECG monitoring, asymptomatic episode interpreted as second-degree atrioventricular block (AVB) Mobitz type II were reported, with pause followed by wide QRS complexes (fig.1). According to 2021 ESC Guidelines, pacing was initially considered. Furthermore, given EF <35%, unclear syncopal history, and LBBB with QRS duration >135 ms, cardiac resynchronization therapy with defibrillator (CRT-D) for primary prevention of sudden cardiac death (SCD) was discussed. However, severe underweight raised concerns regarding increased procedural risk, including device erosion, pocket infection, pneumothorax, and cardiac perforation. Detailed review of telemetry tracings demonstrated an abnormally flat pause baseline and QRS complex identical in polarity and morphology to descending T waves (fig.2), consistent with another ECG artifact displaying isolated T waves without true ventricular depolarization (fig.3). Thus, telemetry malfunction was identified, and the diagnosis of AVB was excluded. Consequently, the indication for pacing was withdrawn. MT will be continued for two months, after which reassessment for CRT-D wireless implantation will be performed