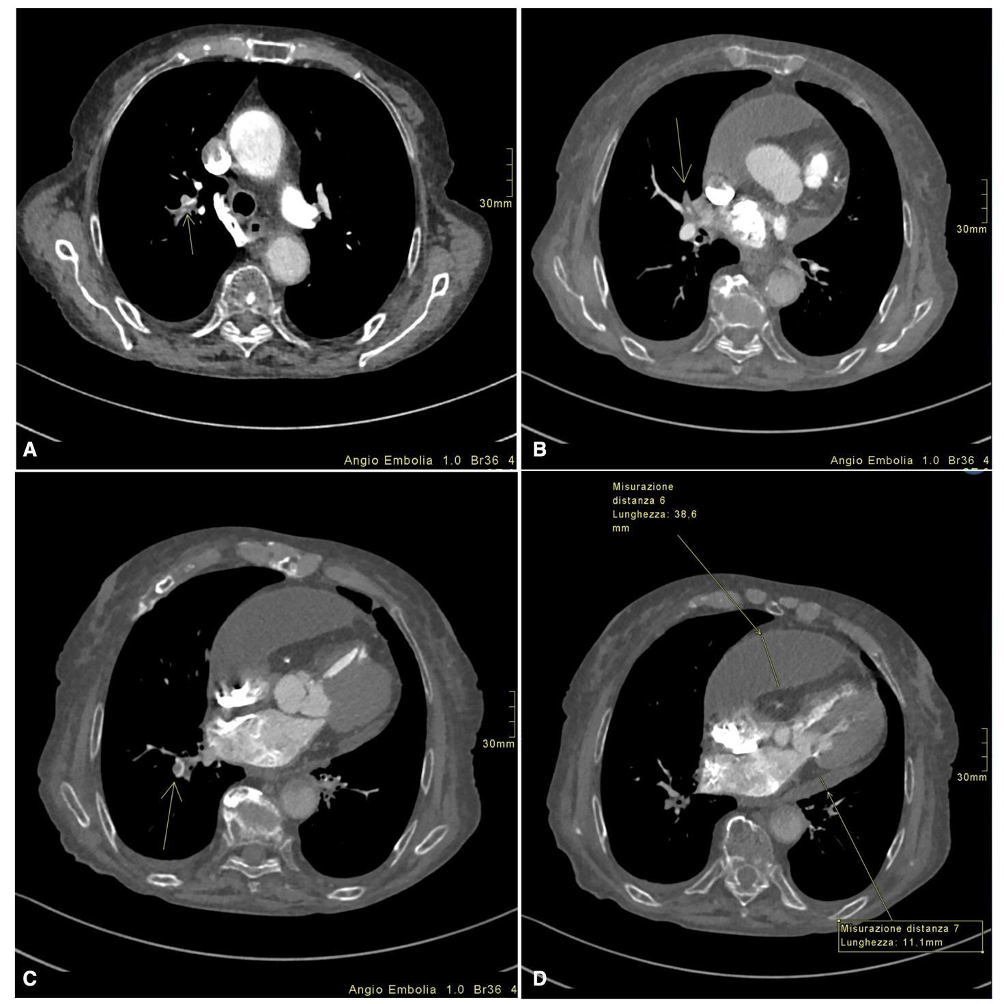
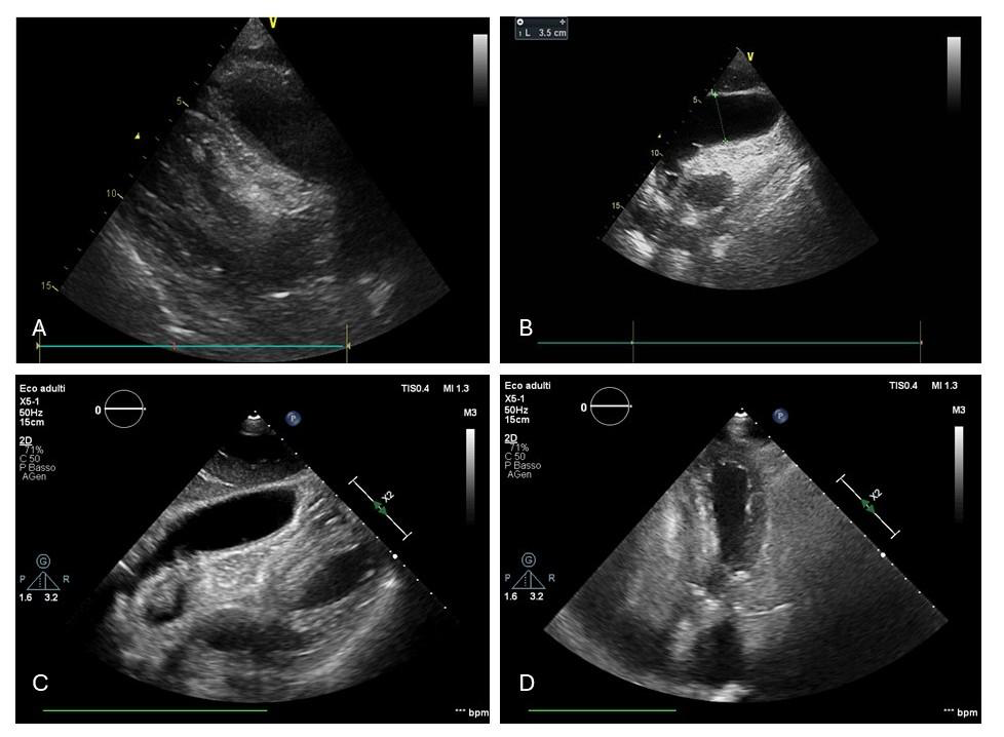
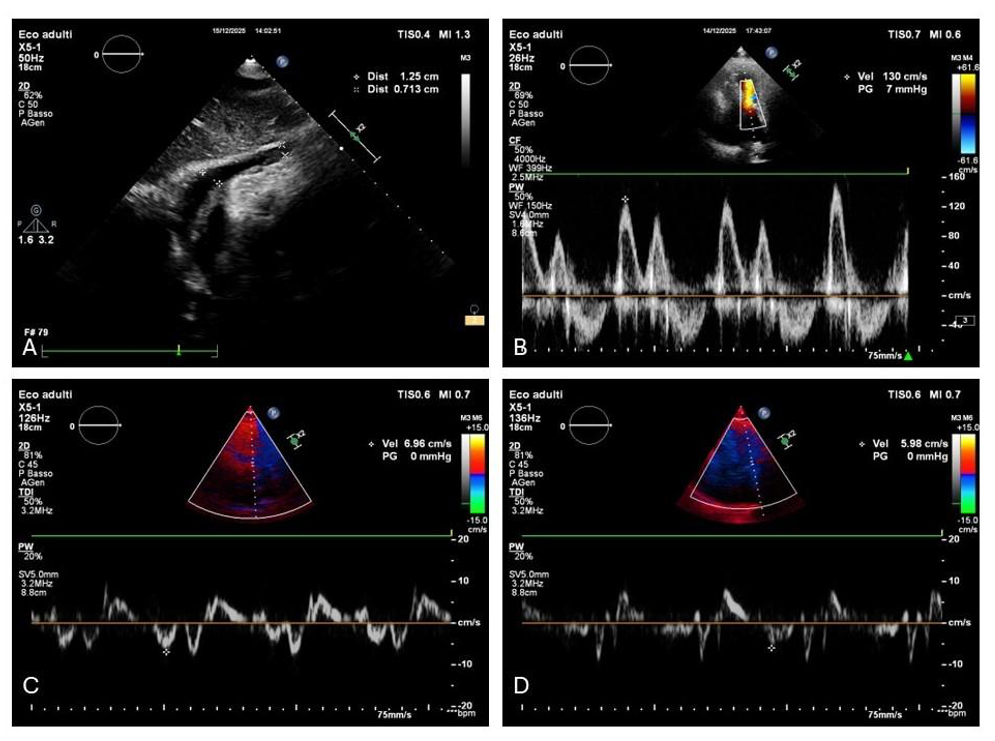
BACKGROUND: Acute pulmonary embolism (PE) is usually suspected when dyspnoea and acute right-ventricular (RV) dysfunction coexist. Chronic loculated pericardial effusion may compress the right chambers and blunt symptoms and RV imaging markers. We report a case in which pericardial compression dominated the haemodynamic picture while a multifocal segmental PE was initially relatively “silent”. CASE PRESENTATION: An 86-year-old woman (COPD, hypertension) with a chronic right-predominant pericardial effusion presented with exertional dyspnoea and leg oedema. ECG showed sinus tachycardia with low voltages. D-dimer and BNP were markedly increased, with mild hs-troponin rise and renal impairment (CrCl ~30 mL/min). CT pulmonary angiography showed multiple segmental thrombi in the right upper, middle and lower lobes, plus a partially loculated pericardial effusion (max 38 mm) with right-chamber compression. Bedside echocardiography suggested pre-tamponade (near-virtual RV, non-collapsing IVC). Echo-guided subxiphoid pericardiocentesis drained ~300 mL haemorrhagic fluid, with rapid recovery and normal RV filling. Anticoagulation was initiated cautiously (reduced-dose enoxaparin, then therapeutic LMWH and edoxaban 30 mg/day). Bilateral proximal DVT was documented; follow-up echo showed mild residual effusion with fibrin and early constrictive physiology. CONCLUSIONS: Right-sided loculated pericardial effusion can mechanically constrain the RV and mask PE-related RV strain. A CT–echocardiography integrated strategy, with reassessment after drainage, helps avoid diagnostic anchoring and supports personalised anticoagulation when thrombotic, bleeding and renal risks coexist.