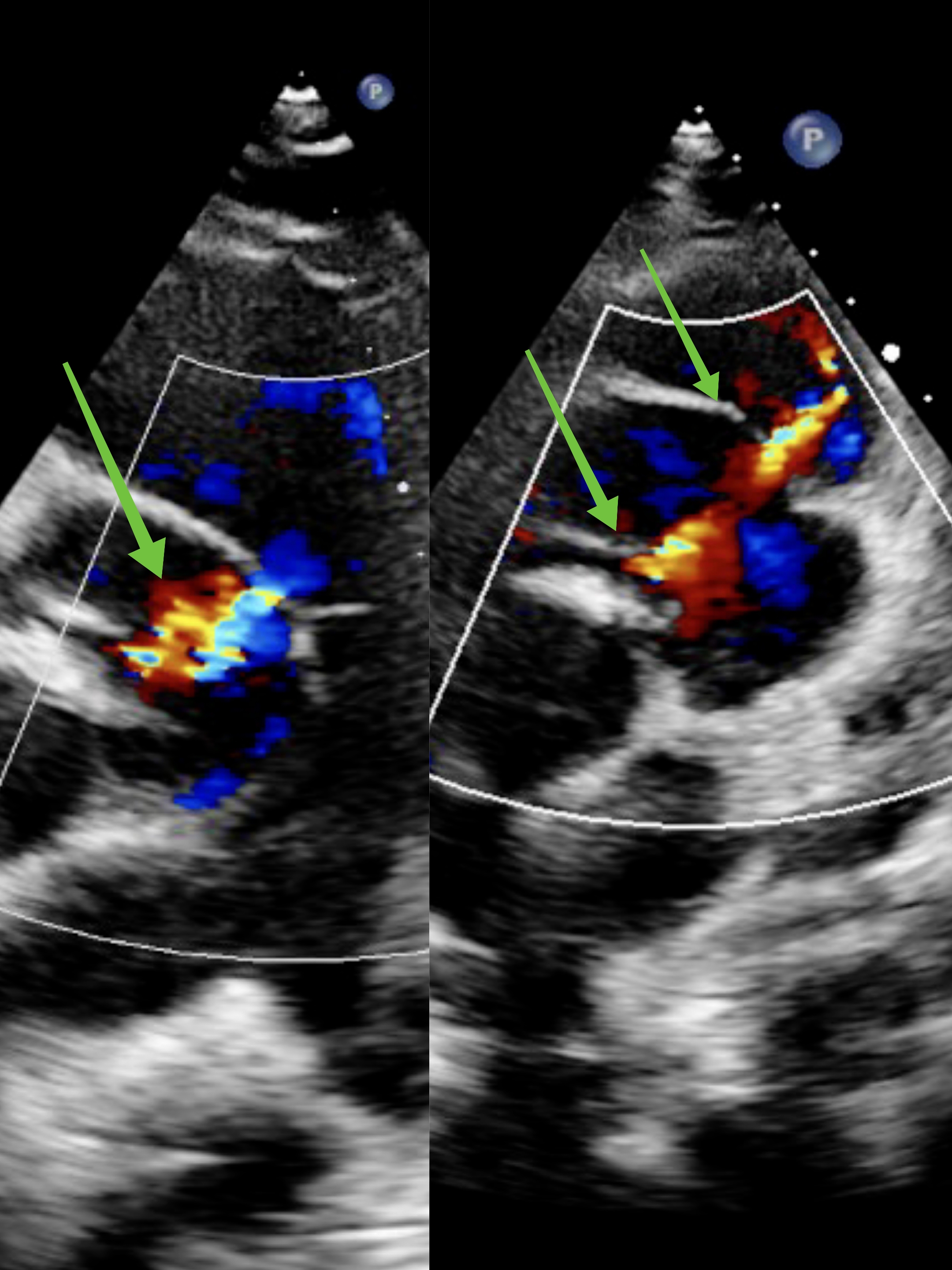
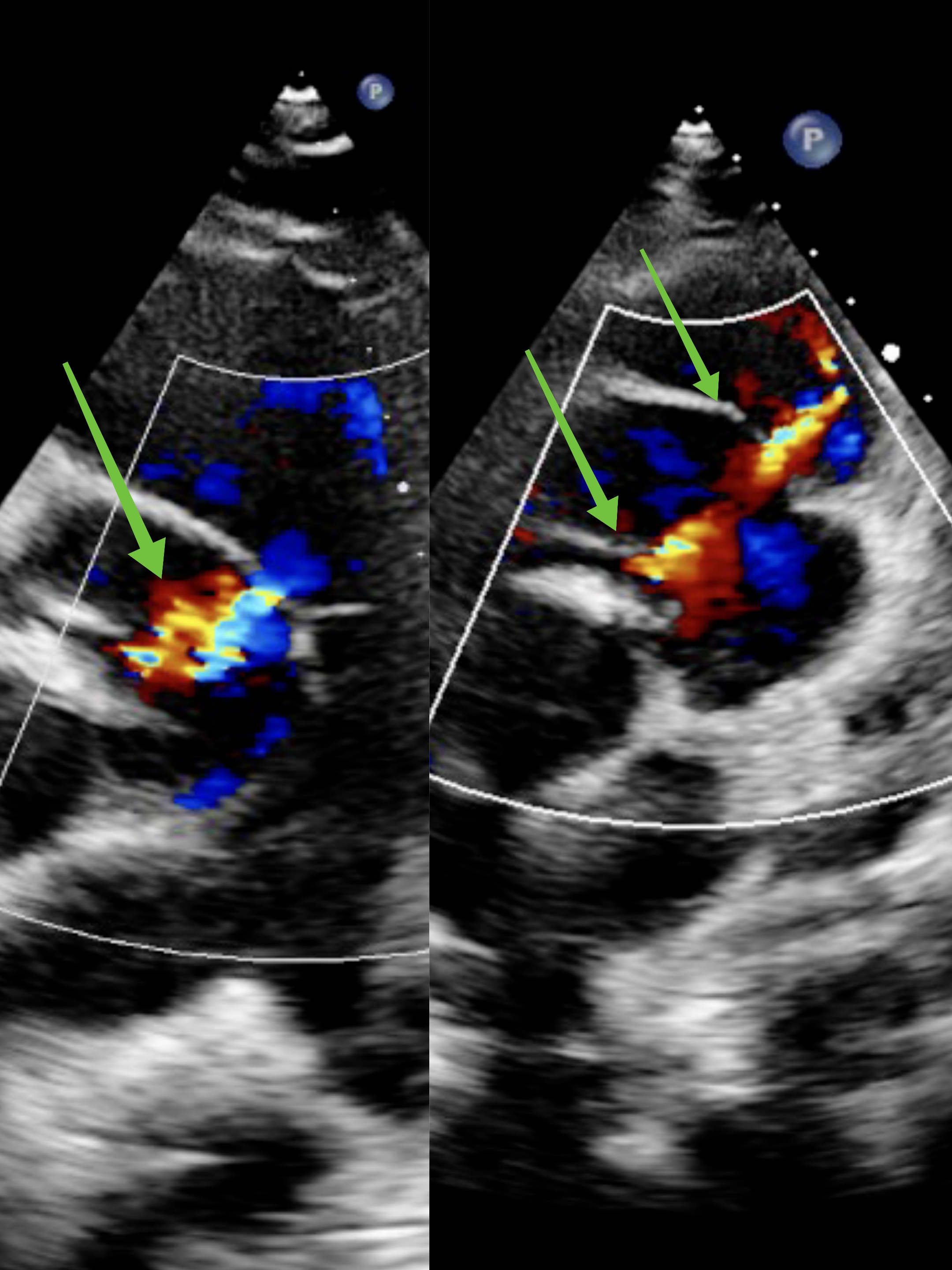
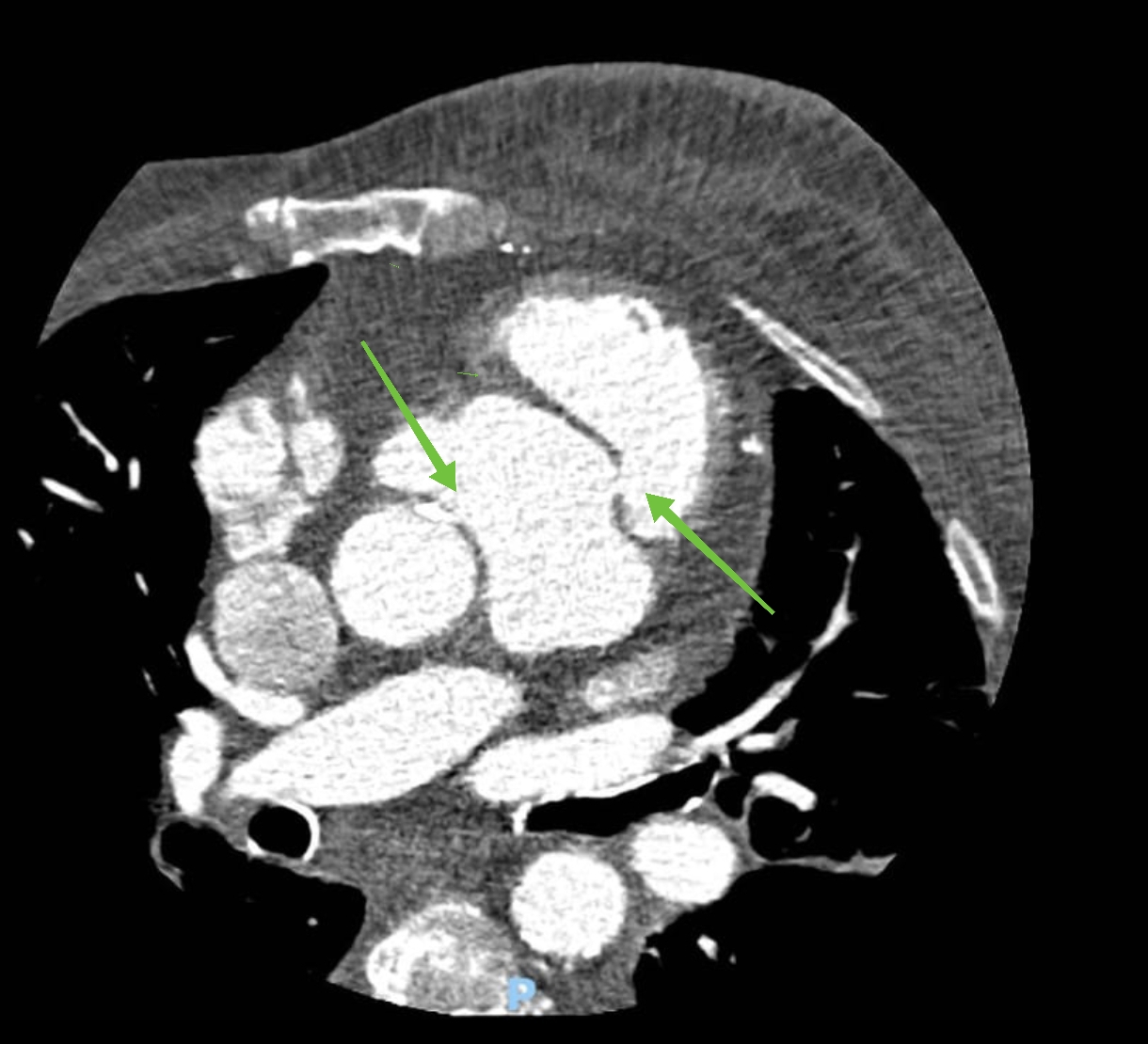
A 76-year-old woman presented with long-standing anasarca. History included chronic ischemic cardiomyopathy with coronary artery bypass (LIMA–LAD), surgical bioprosthetic replacement of severe aortic stenosis and arterial hypertension. Blood tests and abdominal imaging showed liver cirrhosis with marked hypoalbuminemia. Viral, autoimmune, metabolic and alcohol-related causes were excluded, suggesting cardiac cirrhosis. Transthoracic echocardiography revealed normal left ventricular systolic function, right atrial enlargement, a dilated right ventricle (basal diameter 55 mm) with systolic dysfunction (TAPSE 12 mm, S′ 9 cm/s, FAC 25%) and torrential functional tricuspid regurgitation due to leaflet tethering. Parasternal short-axis view showed a right sinus of Valsalva aneurysm bulging into the right ventricular outflow tract. Off-axis views (Fig.1) showed a significant paravalvular leak at 3 o’clock, directed into the aneurysmal right sinus, which had a defect with a jet entering the right ventricular outflow tract, consistent with a left-to-right shunt and right-sided overload. Transesophageal echocardiography (Fig.2) confirmed the paravalvular flow to the right chambers. Cardiac CT showed an acquired pseudoaneurysm of the right sinus of Valsalva with double fistulous communication to the right ventricle, likely due to partial dehiscence of the bioprosthesis (Fig.3). Despite optimized medical therapy, the patient remained in severe right-sided heart failure with advanced liver disease. Because of cardiac cirrhosis and frailty, corrective surgery was deemed prohibitive. She later died from sepsis. This case illustrates how unrecognized sinus of Valsalva pseudoaneurysm with right-ventricular fistula can cause severe right-sided overload and cardiac cirrhosis years after aortic valve surgery. In patients with apparently cryptogenic cirrhosis and prior valve or other heart surgery, a cardiac cause should be actively sought and early multimodality imaging used to detect potentially correctable complications.