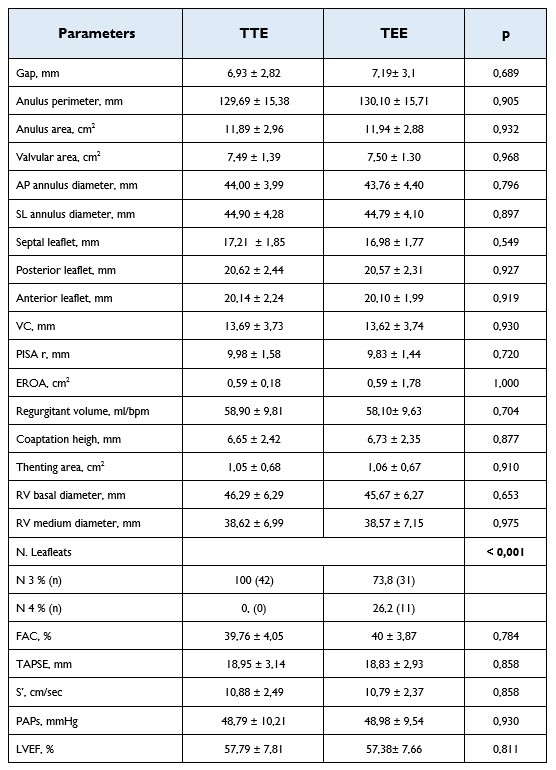
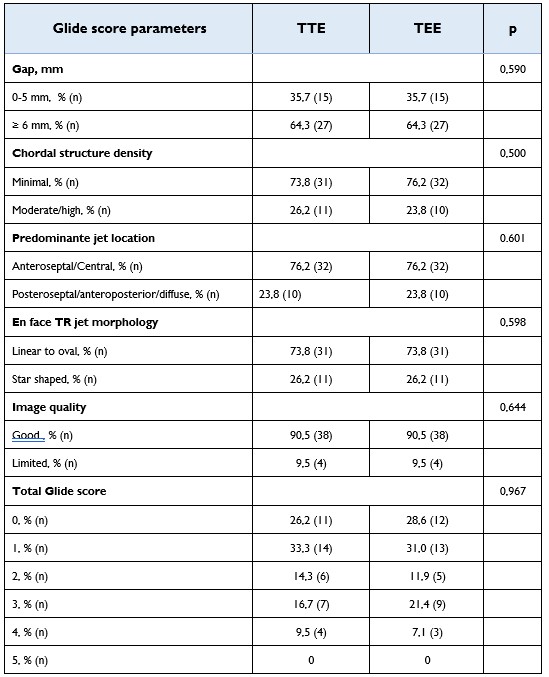
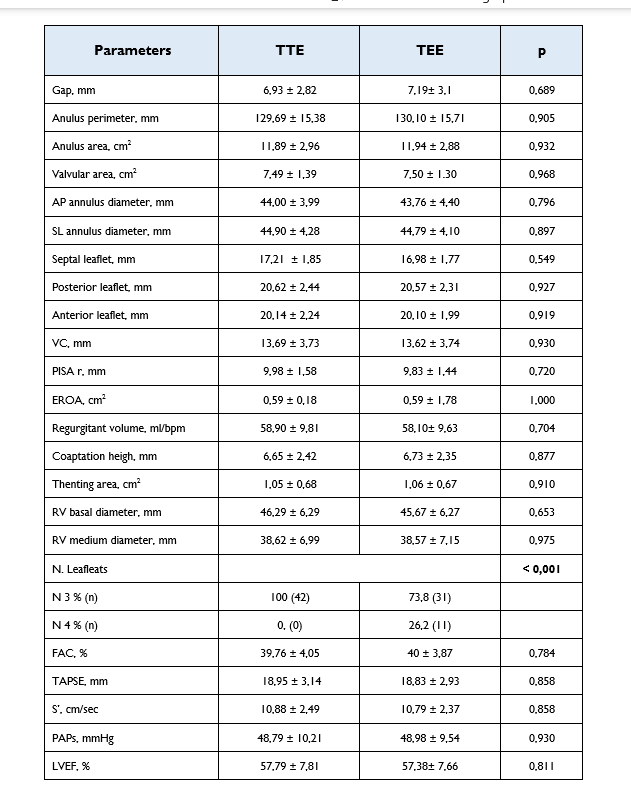
Background: The GLIDE score is a simple five-component scoring system that can be readily obtained during transesophageal echocardiographic imaging and has been shown to predict the likelihood of procedural success with transcatheter tricuspid edge-to-edge repair (T-TEER). Patients with a high GLIDE score (≥4 points) are less likely to benefit from T-TEER and are at increased risk of significant residual tricuspid regurgitation (TR). However, it remains unclear whether transthoracic echocardiography (TTE) alone is sufficient for screening patients considered for transcatheter or surgical interventions, or whether transesophageal echocardiography (TEE) is always required. Aim: The aim of this study was to compare the accuracy of two-dimensional (2D) and three-dimensional (3D) echocardiographic parameters, including the GLIDE score, obtained by TTE versus TEE for screening patients with TR who are candidates for surgical or transcatheter intervention. Methods: Consecutive patients with symptomatic and significant TR were prospectively enrolled. Each patient underwent both 2D/3D TTE and 2D/3D TEE on the same day. The GLIDE score was calculated using both imaging modalities. The score is based on five components: septo-lateral coaptation gap, chordal structure density, TR jet location, en-face TR jet morphology, and image quality. Each component was categorized as either straightforward (0 points) or complex (1 point), resulting in a total score ranging from 0 to 5. Results: The study population included 42 patients (25 men and 17 women) with a median age of 79 years. Of these, 52.3% had severe TR, 42.8% massive TR, and 4.7% torrential TR. No statistically significant differences were observed between TTE and TEE in the assessment of TR severity, right ventricular size and function, annular dimensions, coaptation gap, or overall GLIDE score (all p > 0.05). In contrast, leaflet number was more accurately evaluated by TEE (p < 0.001). Table 1 and 2. Conclusions: Transthoracic echocardiography represents a reliable tool for the initial screening of patients with significant TR who are candidates for surgical or transcatheter intervention. In particular, the GLIDE score can be effectively applied using transthoracic imaging as a first-line screening method. These findings are especially relevant for elderly and frail patients, who may be spared a transesophageal examination when TTE findings already suggest unfavorable anatomy for intervention.