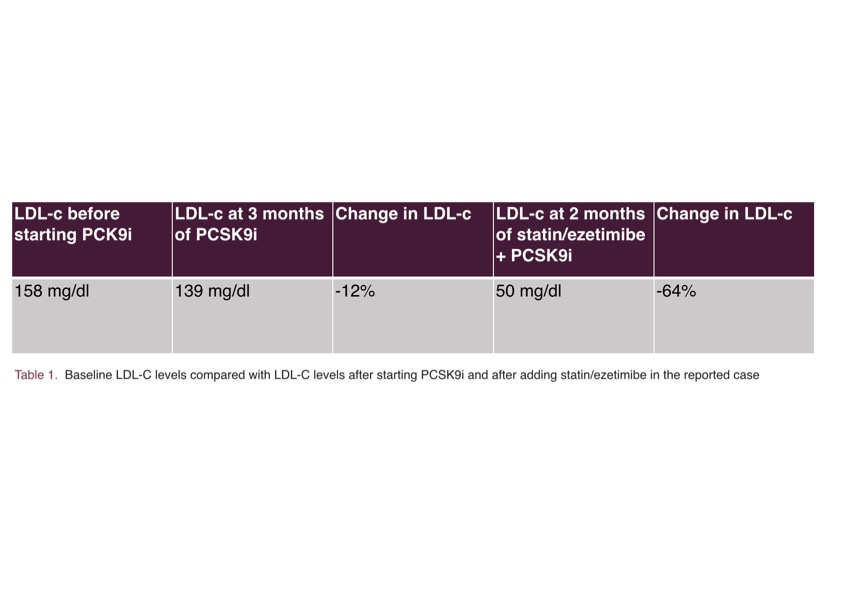
Introduction: The expected response to iPCSK9 therapy in terms of LDL-C reduction is around 60% in monotherapy. In this clinical case we present an example of hyporesponse to therapy with monoclonal antibody (alirocumab) used in monotherapy. Presentation of the case: Patient F, 77 years old, hospitalized in march 2018 for lateral STEMI treated with PTCA + DES on occluded proximal Cx. Calculated LDL 188. Discharged with atorvastatin 80 mg. October 2018 new hospitalization for TIA. Doppler carotids ultrasound showed stenosis 40% left ICA. She was discharged with simvastatin 40/ezetimibe 10 mg due to intolerance to atorvastatin (myalgia). She presented unchanged LDL values for early self-suspension of statin therapy. CK within limits. Subsequent regular cardiological follow up. The therapy was remodified during follow up for intolerance to simvastatin 40 mg and also rosuvastatin 5 mg. Ezetimibe was also suspended due to reported myalgia. In May 2023 Praluent 75 mg 1 fl every 2 weeks was then prescribed with a starting LDL of 158. At the check-up of July 2023 unchanged LDL was persisting, due to poor therapeutic adherence. In october 2023 for LDL value of 139, in this case with constant therapy, Praluent was increased to 150 mg. In december 2023: LDL 137. A rechallenge of statin therapy was then proposed (rosuvastatin 5 mg in the morning every other day, plus ezetimibe 10 mg), the patient being motivated for treatment and in the absence of available alternatives. After 2 months LDL cholesterol was calculated at 50 mg/dl in the absence of muscular symptoms. Characteristics of the patient: Treatment naive upon admission. Lack of family history of early CV disease. Negative CV objective, no xanthomas. Former mild smoking. TSH within limits. Lp(a) within limits. Discussion: The pivotal studies of alirocumab and evolucumab showed significant results in terms of reduction of LDL cholesterol in patients with previous ACS and chronic ischemic heart disease. The variability of response when used as monotherapy is not known in clinical practice, however a minor effect can be expected due to the lack of synergistic effect between different lipid-lowering therapies. In this clinical case of probably polygenic hypercholesterolemia in secondary prevention in patient with previous intolerance to statins and ezetimibe, rechallenge of therapy was attempted with satisfactory results, demonstrating the importance of the therapeutic association.