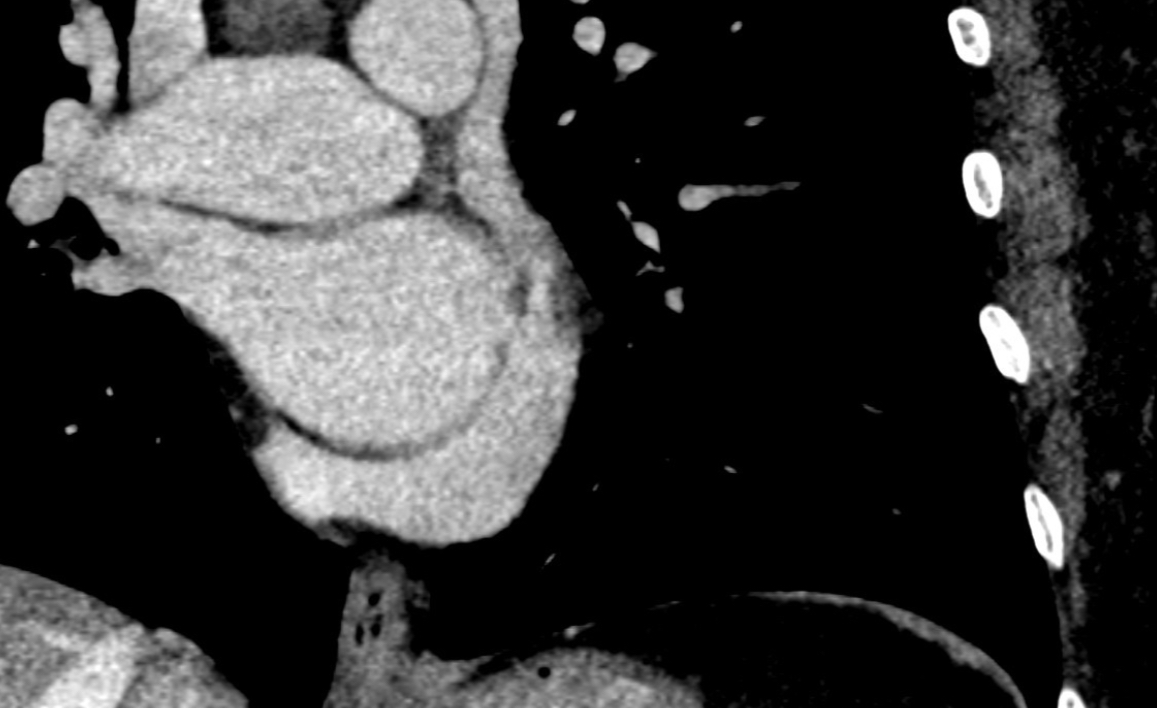
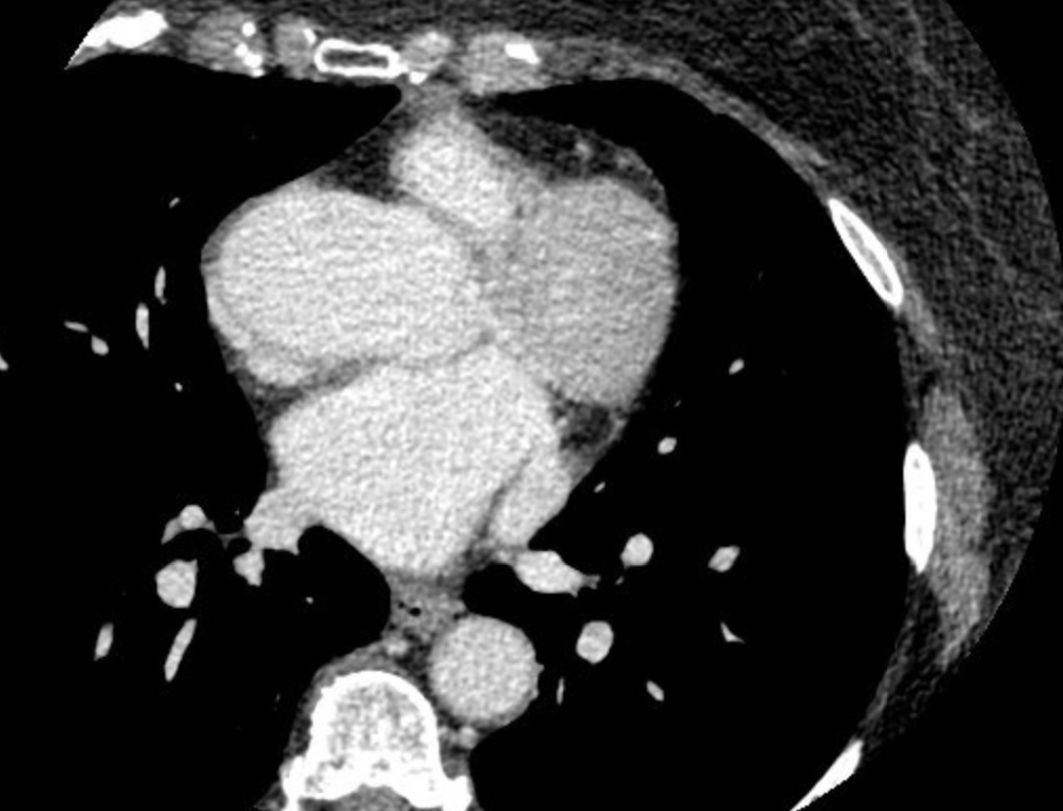
INTRODUCTION Unroofed coronary sinus is a rare congenital heart anomaly and the most unusual type of atrial septal defect with nonspecific clinical manifestations. CASE REPORT A 73-year‐old woman presented to the Emergency Department for palpitations and chest pain. She had History of recurrent palpitations and a previous access to the Emergency Room with electrocardiogram (ECG) evidence of supraventricular tachycardia with wide QRS left bundle block-type, treated with intravenous infusion of amiodarone. Physical examination revealed rhythmic cardiac activity and normal vital signs. The ECG showed sinus rhythm with isolated premature atrial beats, normal atrioventricular conduction, normal QRS and normal ventricular repolarization, without signs of ischemia. Troponin was negative. The patient therefore underwent an electrophysiological (EP) study which showed, in basic conditions, a sinus rhythm with normal conduction intervals, numerous isolated atrial ectopic beats with distal-proximal activation on the coronary sinus (CS). The study also demonstrated non-inducibility of supraventricular tachycardia or atrial fibrillation. During the EP study, an atypical manipulation of the decapolar catheter in the CS gave suspicion of an anomaly of this structure. Further imaging investigations were performed. A transesophageal echocardiogram showed marked dilation of the coronary sinus and, during infusion of microbubbles from the brachial vein, an immediate passage of microbubbles in the left atrium with apparent integrity of the interatrial septum was observed. At last the patient underwent Cardiac CT that documented the absence of the CS roof at the level of the superior-posterior wall with a communication between the CS and the left atrium; in addiction the presence of a persistent left superior vena cava (PLSVC) which continued into the coronary sinus was evidenced. Final diagnosis of unroofed-coronary-sinus was made. DISCUSSION Unroofed coronary sinus is a rare type of atrial septal defect (ASD) and is caused by complete or partial absence of the CS roof, leading to a connection between CS and left atrium. It usually involves various anatomical characteristics depending on the location of the unroofed portion of the CS and ASD. This defect accounts for less than 1% of ASDs and is commonly associated with a PLSVC which is present in 75% of unroofed CS cases. It is often difficult to make an accurate diagnosis of unroofed CS with conventional echocardiography.