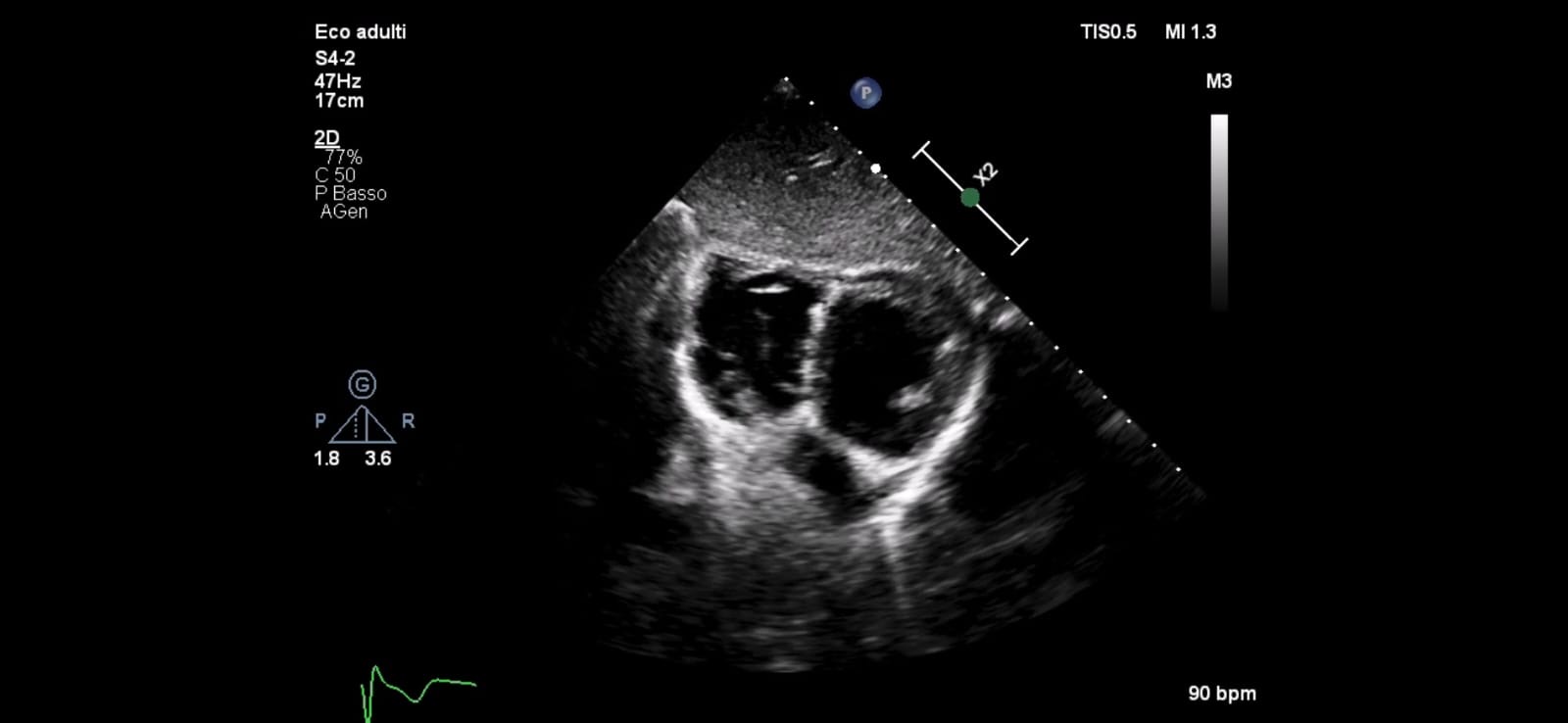
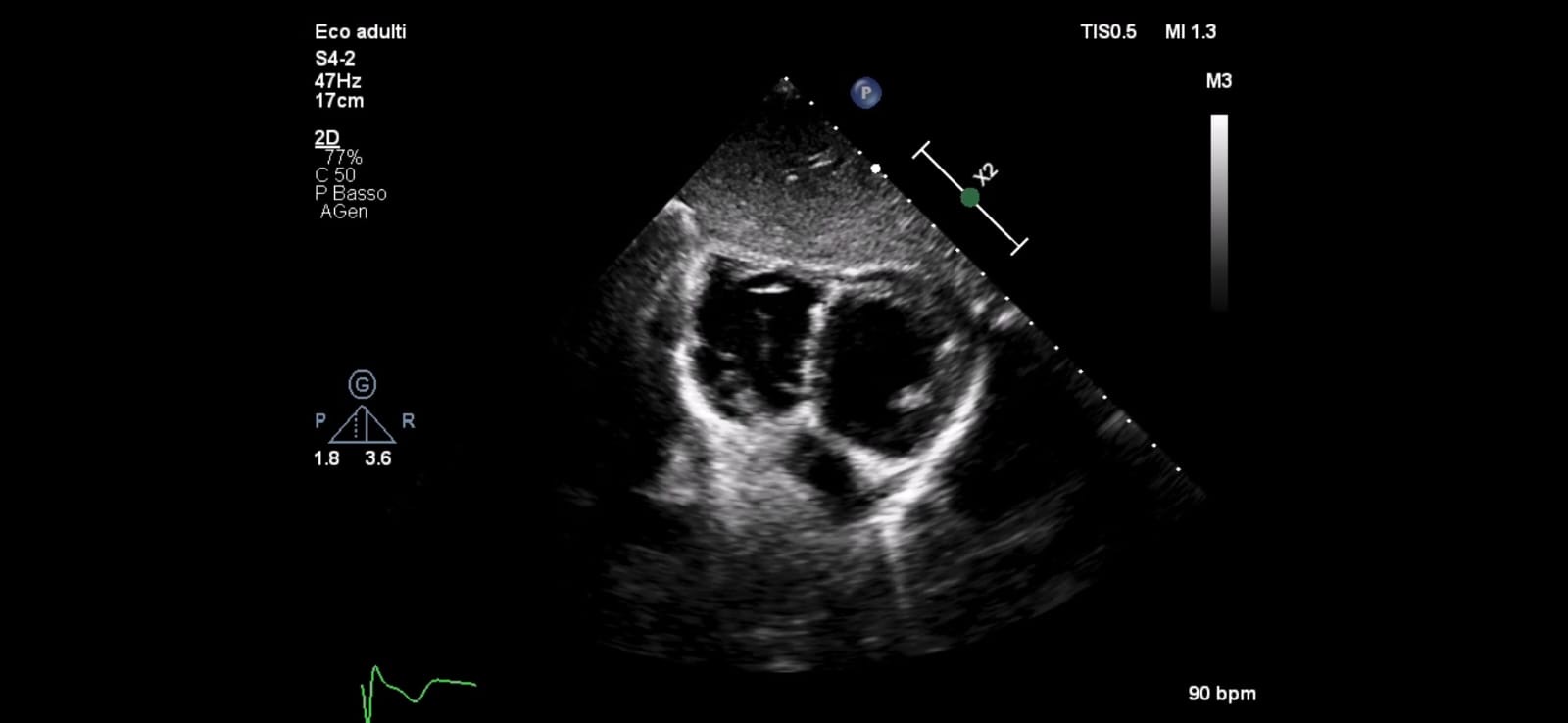
We present the case of a 7-year-old child who was suspected of having dilated/hypertrophic cardiomyopathy of the right ventricle (RV) based on prenatal ultrasound findings. He was admitted to our department at birth, where echocardiography revealed hypokinesia in the inferior and anterior walls of the RV, along with an aneurysm in the basal segment of the RV's free wall. He showed no symptoms or EKG abnormalities. The hospital stay was uneventful. At the age of four, MRI revealed a slightly dilated and dysmorphic RV, characterized by hypertrophy of the moderator band, resembling a milder form of a 'Double Chambered Right Ventricle (DCRV)’, preserved contractility (EF = 52%) and the absence of fibrosis. The other cardiac chambers appeared normal. By the time of our evaluation at seven years old, he had experienced normal growth without any limitations. The echocardiogram confirmed that RV was trabeculated, with a diverticulum in the anterior wall, preserved contractility without systolic bulging or right ventricular outflow tract obstruction (RVOTO), with estimated pulmonary artery pressures of 20 mmHg. The EKG doesn’t show signs of RV overload. Regular follow-up was recommended along with 24-hour ECG Holter monitoring to evaluate any potential arrhythmic burden. He was encouraged to maintain an active lifestyle without limitations. DCRV is a rare congenital heart defect characterized by an abnormal muscular band that divides the RV into two cavities, potentially leading to a pressure gradient between the inflow and outflow regions. The condition is primarily diagnosed through echocardiography, especially in children, but MRI provides superior resolution. DCRV is often associated with ventricular septal defects, pulmonary valve stenosis, double-outlet RV, and tetralogy of Fallot. Most cases are diagnosed in childhood for evaluation due to cardiac murmurs. In the absence of RVOTO this condition remains asymptomatic for a long time, as seen in our case. Surgical intervention typically involves resecting the obstructing muscular bundles and is recommended when symptoms or an associated lesion or a significant degree of asymptomatic obstruction are present. The RVOTO observed in DCRV may progress, leading right heart failure symptoms. Literature indicates that surgical outcomes and long-term postoperative prognosis are favorable, with no reported recurrence of DCRV or fatal arrhythmias during extended follow-up periods.