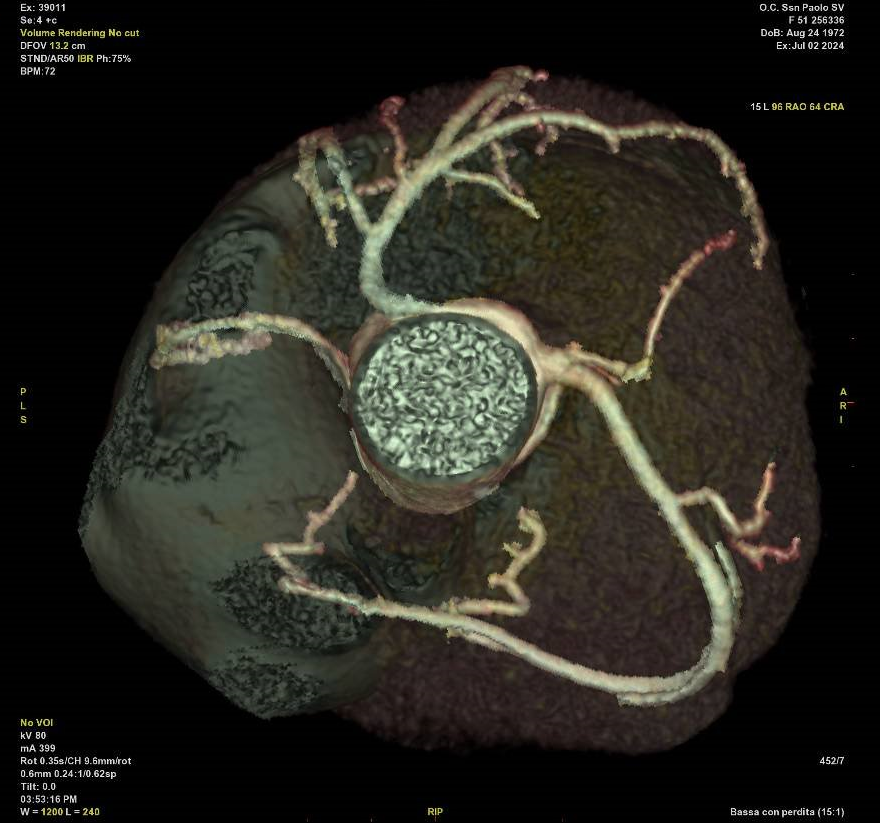
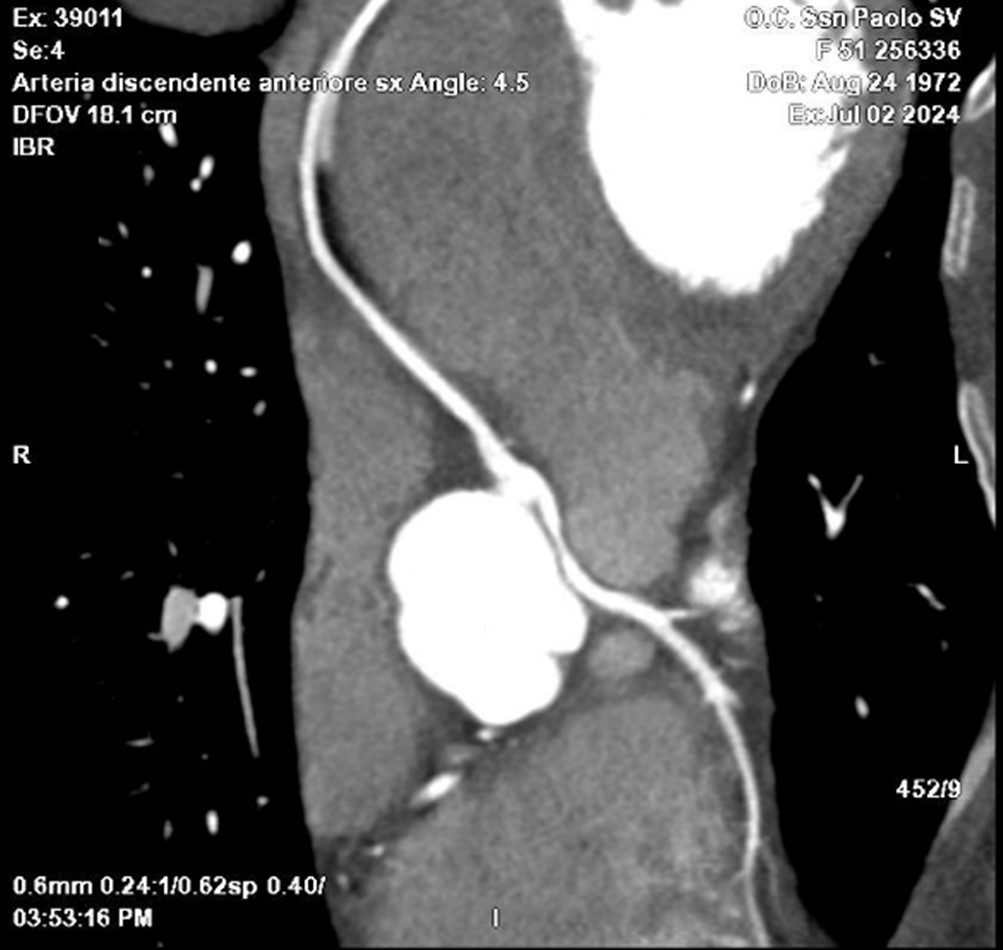
Background: Anomalous aortic origin of coronary arteries (AAOCA) is a rare condition that may occur as an isolated anomaly or with other congenital heart defects. Often asymptomatic, AAOCA can cause myocardial ischemia, arrhythmias, or sudden cardiac death, especially when associated with coronary origin from the opposite sinus of Valsalva (SoV), interarterial course, intramural segment, high ostium, or sharp take-off angle. Diagnosis is challenging: suspicion often arises during coronary angiography, while advanced imaging confirms the diagnosis and identifies high-risk features. Surgery is recommended for symptomatic cases and may be considered for asymptomatic patients with inducible ischemia or high-risk anatomy. Case Description: A 63-year-old woman with diabetes and hypertension was admitted to San Paolo Hospital (Savona) for fatigue and transferred to Cardiology for a new diagnosis of heart failure with mildly reduced left ventricular ejection fraction (LVEF), moderate mitral regurgitation, and moderate aortic stenosis and regurgitation. Soon after admission, she developed acute pulmonary edema, treated with diuretics and non-invasive ventilation. Once stabilized, a coronary angiography, with intravascular ultrasound and a coronary CT, revealed no significant coronary stenoses but showed an angulated origin of the left main stem from the right SoV with an interarterial course between the aorta and pulmonary artery, causing mild lumen narrowing. Additionally, the slender circumflex artery originated from the right SoV. The patient was referred to San Martino Hospital (Genoa) for cardiac surgery, including a left internal mammary artery bypass to the left anterior descending artery and replacement of the mitral and aortic valves with biological prostheses. The postoperative course was complicated by wound bleeding requiring re-exploration, anemia, and transient sinoatrial block. However, she was discharged after 31 days and was asymptomatic at 3 month follow-up. Echocardiography showed LVEF recovery to 58% and mildly increased gradients across both prostheses. Conclusions: AAOCA is a rare yet potentially lethal cause of myocardial ischemia and left ventricular dysfunction, particularly when linked to high-risk anatomical features. Advanced imaging is pivotal for risk stratification and guiding management. Surgery is indicated in symptomatic patients or those with high-risk anatomy, particularly when coexisting anomalies are surgically correctable.