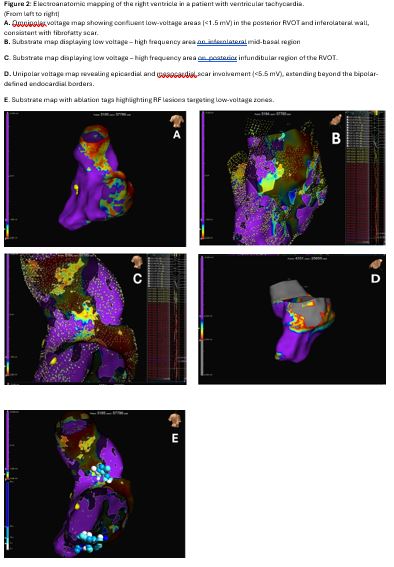
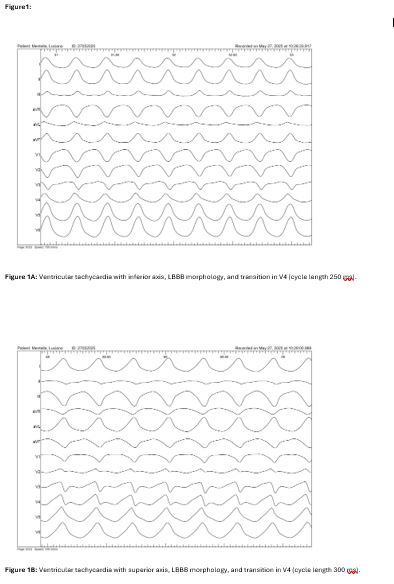
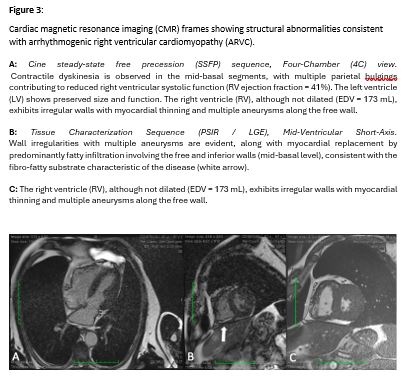
Background: Ventricular tachycardia (VT) with a left bundle branch block (LBBB) morphology and inferior axis is classically associated with idiopathic right ventricular outflow tract (RVOT) arrhythmias. However, overlapping electrocardiographic patterns may conceal an underlying arrhythmogenic cardiomyopathy, particularly when multiple VT morphologies coexist. Case Presentation: A 61-year-old man presented to the emergency department with acute palpitations and diaphoresis. Twelve-lead ECG revealed a hemodynamically unstable wide-complex tachycardia at 250 bpm, promptly terminated by electrical cardioversion. Coronary angiography excluded ischemic heart disease. The arrhythmia morphology (LBBB, inferior axis, V4 transition) initially suggested idiopathic RVOT-VT. Electrophysiological Study and Mapping: High-density electroanatomic mapping of the right ventricle identified discrete low-voltage regions in the posterior RVOT and inferolateral mid-basal right ventricle, predominantly meso-epicardial on unipolar mapping. Programmed ventricular stimulation induced two distinct VT morphologies: one with inferior axis (cycle length 250 ms) and a second with superior axis (cycle length 300 ms). Pace mapping showed >92% concordance with both VTs. Targeted radiofrequency ablation rendered the arrhythmias non-inducible. Imaging and Diagnosis: Cardiac magnetic resonance demonstrated right ventricular fibrofatty replacement, free-wall aneurysms, regional dyskinesia, and mildly reduced right ventricular ejection fraction (41%). Integration of clinical, electroanatomic, and imaging findings fulfilled two major Padua criteria, confirming a diagnosis of arrhythmogenic right ventricular cardiomyopathy. Management and Conclusions: A dual-chamber implantable cardioverter-defibrillator was implanted for secondary prevention. This case highlights how dual VT morphologies and advanced electroanatomic mapping can reveal concealed arrhythmogenic cardiomyopathy masquerading as idiopathic RVOT-VT. Multimodal integration is essential for accurate diagnosis and risk stratification in complex ventricular arrhythmias.