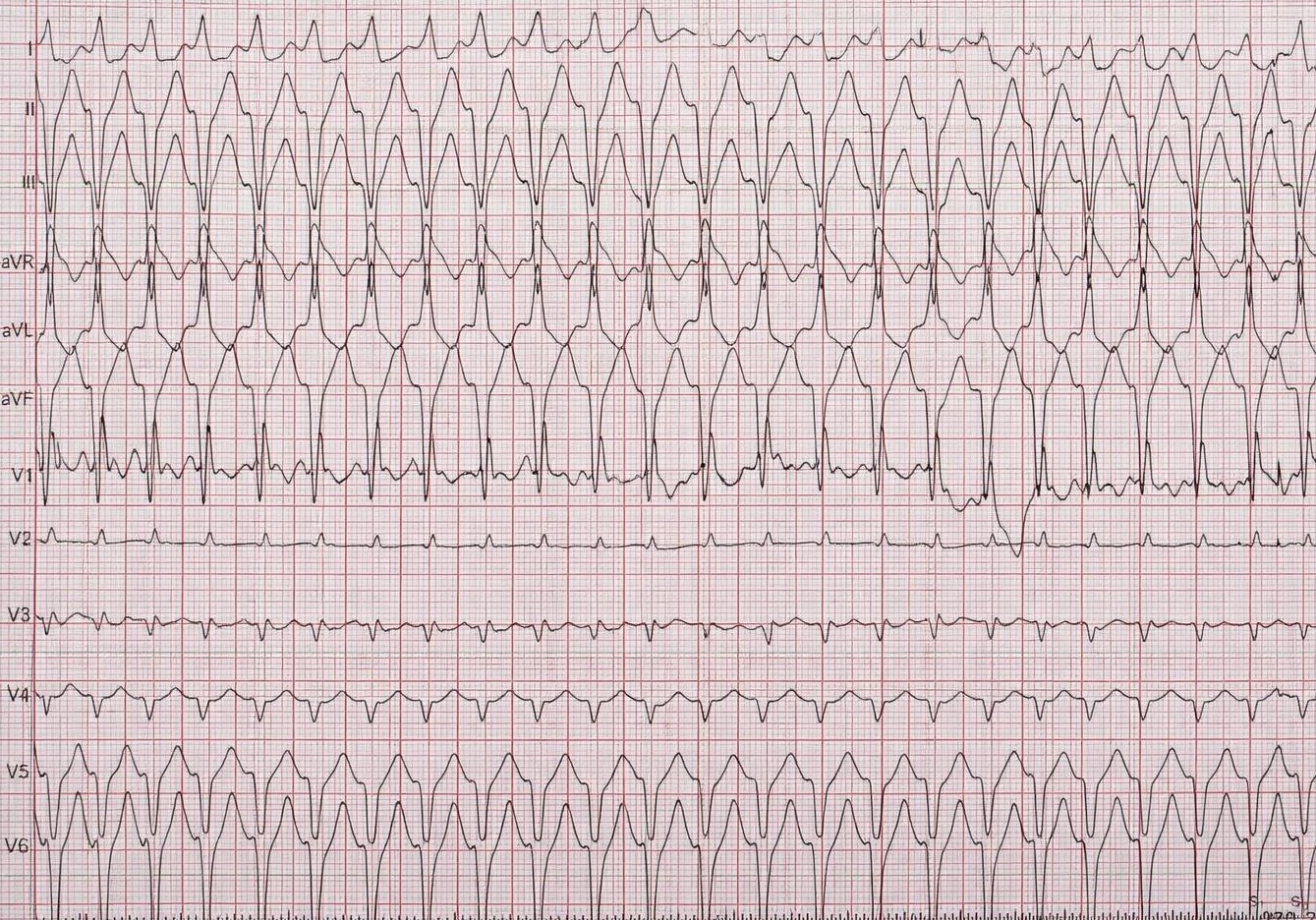
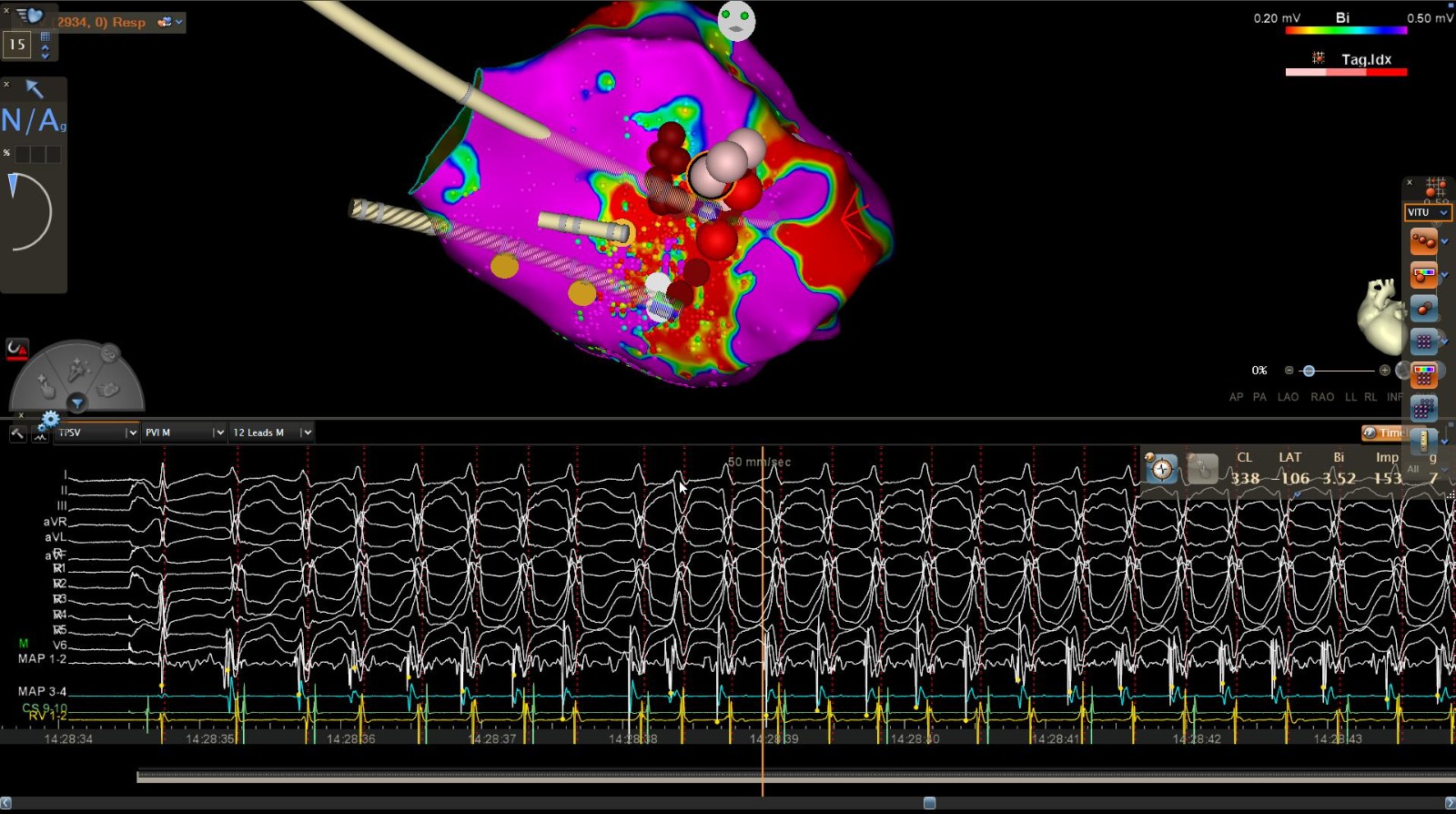
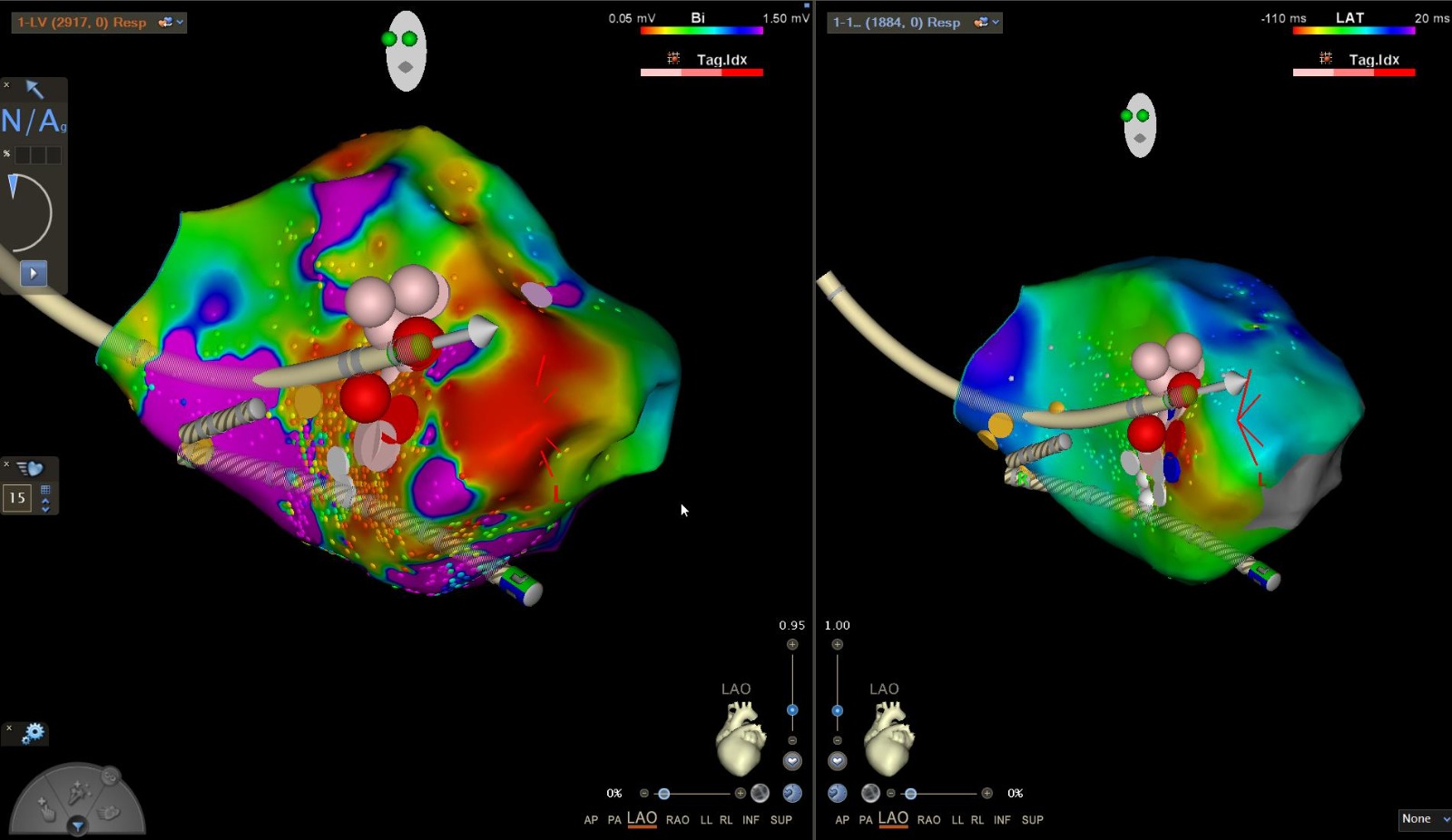
A 76 y.o. patient presented to E.R. after the onset of dyspnea. The ECG showed a tachyarrhythmia (QRS width 115 ms) at 150 bpm with LAFB and a RBBB morphology, with regularly inscribed P within the QRS. Electrical cardioversion was performed, restoring SR with persistent deep negative T waves in the inferoseptal leads. The patient reported prior palpitations and history of paroxysmal AF treated with flecainide (pill-in-the-pocket). Therefore, atrial flutter conducted with aberrancy was hypothized. Given the elevated troponin values and persistent repolarization abnormalities, coronary angiography was performed, revealing critical stenosis of the mid-LAD, which was treated with PTCA + stenting. During hospitalization, ECG monitoring revealed several episodes of the original arrhythmia, resistant to infusion of Amiodarone and to implementation of beta-blockers and subsequent switching to nonDHP Calcium Channel Blockers. Therefore, after pharmacological washout, an EP study was indicated. Using a programmed stimulation protocol, the clinical tachycardia was induced (double extrastimulus). However, the signals revealed the presence of a ventricular arrhythmia with fixed retrograde atrial conduction. Morphology was consistent with posterior fascicular VT, then a subsequent transaortic approach was used to perform mapping of the LV chamber. In the inferior septal area, inert tissue attributable to an ischemic scar was identified. Near this area local LAVA and during tachycardia pre-sistolic potential EGM with a – 45 ms activation timing and an unipolar QS were found. Therefore, RF energy (35 W) was applied in this zone, resulting in complete non-inducibility even after 20 minutes when protocols were repeated. At 6 month follow-up, there was not recurrence of tachycardia. Discussion: The presence of tachycardia with RBBB + LAFB and a not broad QRS should not rule out a VT, especially fascicular types, whose features are characteristic (they represent about 10% of idiopathic VT). Furthermore our specific case was a reentry circuit ventricular tachycardia on an ischemic scar basis, with exit site near the posterior fascicle. Morphology was related to exit site, but the existence of a reentry circuit explained its resistance to nonDHP CCB. Differential diagnosis with a SV tachyarrhythmia in our case was more difficult by the history of paroxysmal atrial fibrillation and the inducibility of arrhythmia despite flecainide, consistent with an ischemic etiology.