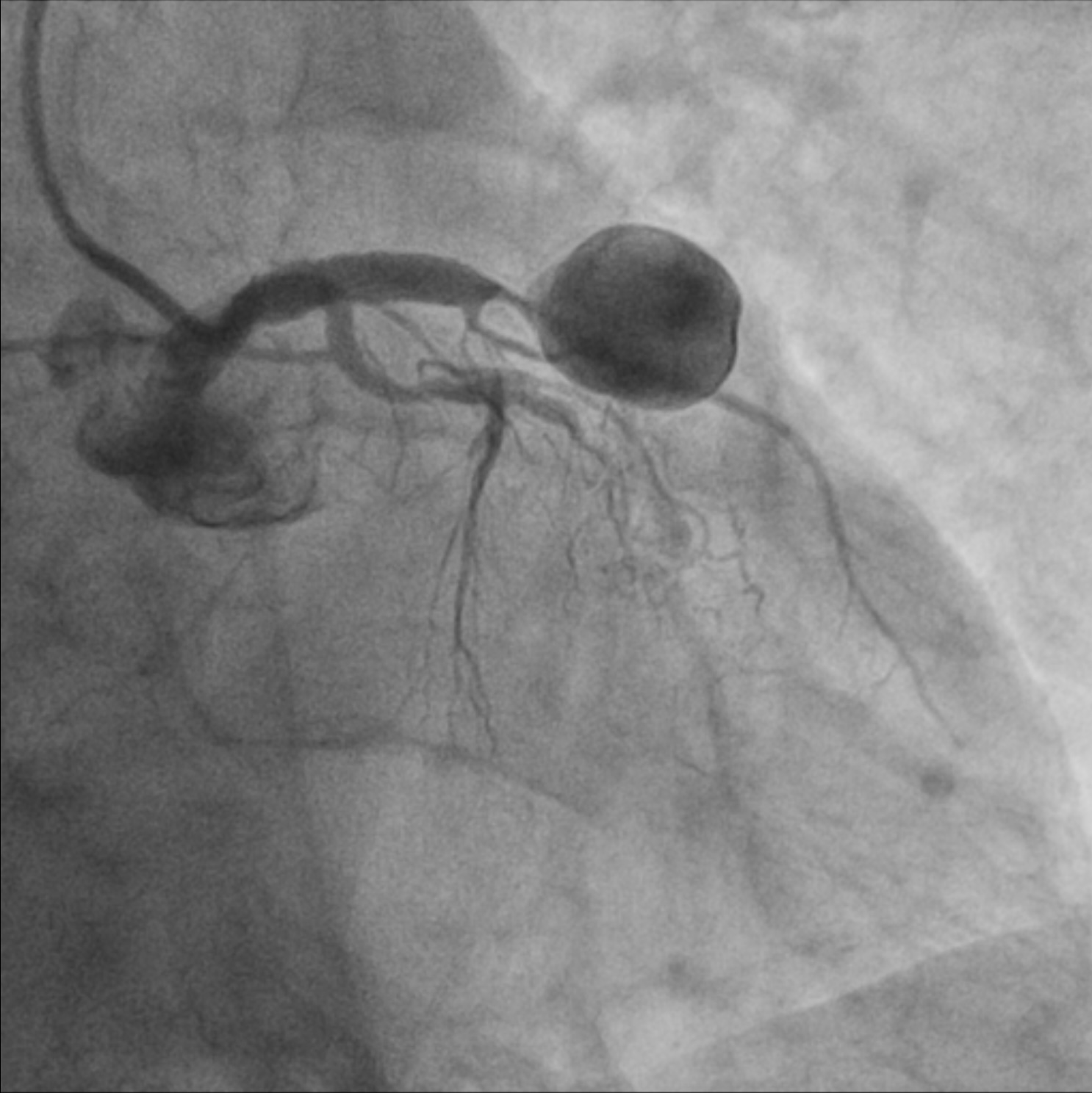
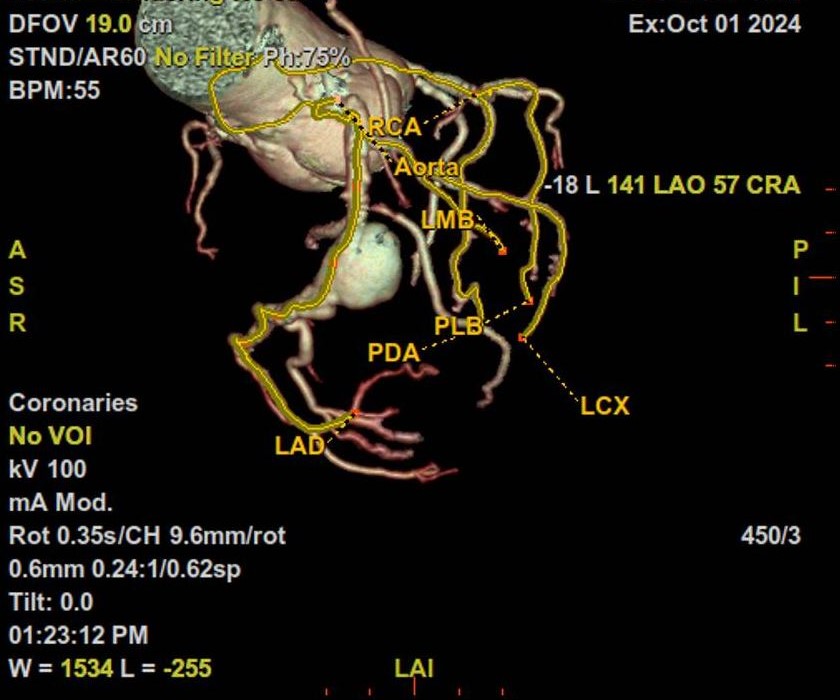
An 82-year-old Caucasian patient was admitted to the surgical department for an endoscopic retrograde cholangiopancreatography due to an ampullary tumor of the Vater's papilla. Medical history includes: active smoking, abdominal aortic aneurysm below the renal arteries and chronic kidney disease. During routine preoperative evaluations, symmetric inverted T waves were noted on the ECG, prompting a cardiological assessment. A coronary CT angiography revealed an ectatic right coronary artery (RCA) with two focal stenoses caused by hypodense (soft) plaques. The left main coronary artery was patent. The left anterior descending artery (LAD) was patent with a 65% focal stenosis in the mid-segment, just upstream of a large aneurysm (maximum dimensions 17×15 mm). The circumflex artery was narrow, with a 90% stenosis in the second segment. An echocardiogram demonstrated normal biventricular wall motion without significant valvular abnormalities. A follow-up cardiological evaluation indicated the need for coronary angiography which documented, in particular, a severe proximal stenosis of the left anterior descending artery, confirming the presence of a large aneurysm with post-aneurysmal subocclusion. Based on the angiographic findings, the patient was indicated for CABG with evidence of an intramyocardial aneurysmal sac, partially calcified, in the proximal LAD. Subsequently, a T-L anastomosis was constructed between the left internal mammary artery and the LAD. The patient was discharged following a good postoperative course without complications. A coronary aneurysm is a focal and pathological dilation of a segment of a coronary artery, exceeding 50% of the vessel's normal diameter. It is a rare condition, with a prevalence ranging from 0.3% to 5% among patients undergoing coronary angiography. Coronary aneurysms can be congenital or acquired and are most commonly found in the LAD, followed by the RCA. Atherosclerosis is the most common cause in adults, followed by Kawasaki disease, connective tissue disorders and infections. Many coronary aneurysms are asymptomatic and are discovered incidentally during examinations for other conditions, as in our case. However, in some cases, they may present with angina, myocardial infarction, or aneurysm rupture. Coronary angiography is the gold standard for diagnosis, while coronary CT is useful for a detailed assessment of size, shape, and calcifications. In most cases, treatment involves performing CABG.