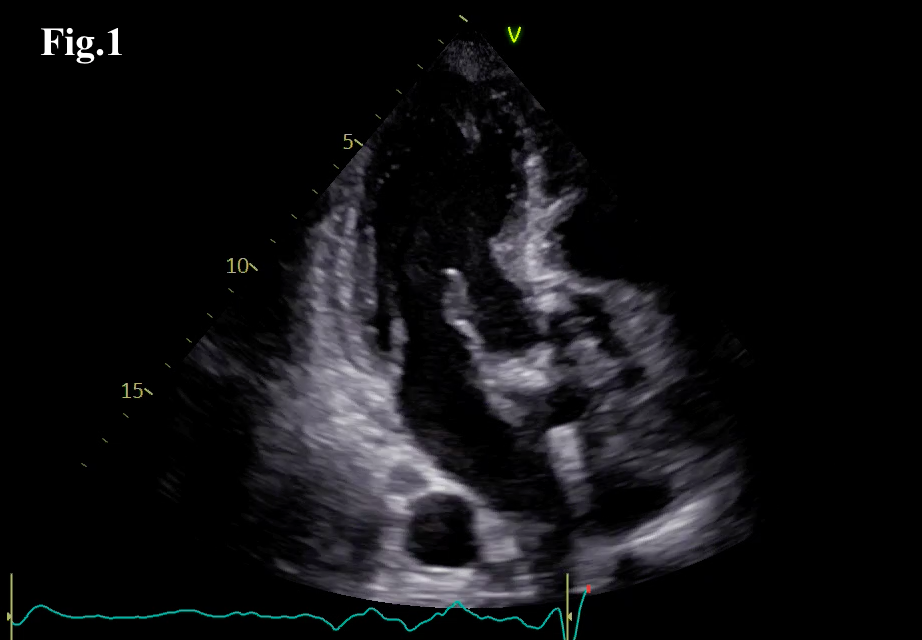
Infective endocarditis (IE) is an infection of the endocardium caused by bacteria or, less frequently, fungi, with an incidence of 3–10 cases per 100,000 people/year. Prosthetic valve endocarditis accounts for 20–30% of cases. Fungal IE is rare (2–4%) but severe, with mortality exceeding 50%. Candida species are most common, followed by Aspergillus, which represents 20–25% of fungal cases. Aspergillus endocarditis is characterized by an insidious course, frequent negative blood cultures, and a high risk of embolic complications, often delaying diagnosis. Clinical case: A 72-year-old man with a history of aortic valve replacement using an Inspiris Resilia Edwards 25 bioprosthesis one year earlier was admitted for persistent fever and gastrointestinal symptoms. Due to ongoing fever and visual impairment, he was transferred to our hospital. Transesophageal echocardiography (TEE) revealed a mobile, pedunculated mass (2 × 1.5 cm) on the posterior aortic side of the prosthetic cusps and additional hypoechoic areas at the sinotubular junction. Moderate prosthetic stenosis (Vmax 3.2 m/s, mean gradient 34 mmHg) with mild central regurgitation was observed. A repeat TEE showed large, irregular, mobile vegetations up to 3.5 × 2 cm, thickening of the posterior prosthetic ring and mitro-aortic junction consistent with a prosthetic abscess, and increased prosthetic mobility. Microbiological investigations confirmed Aspergillus sepsis, and antifungal therapy was initiated. Brain CT performed for neurological symptoms revealed a right rolandic cisternal hemorrhage compatible with septic embolization. Given persistent sepsis, large vegetations, and embolic risk, the patient underwent surgical replacement of the aortic valve with a bioprosthesis. Conclusions: Multimodal imaging is crucial for diagnosing IE and detecting complications. In patients with valve prostheses, TEE remains fundamental for both diagnosis and therapeutic decision-making.