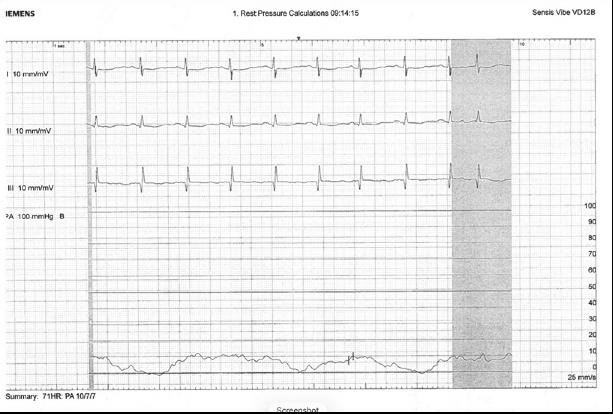
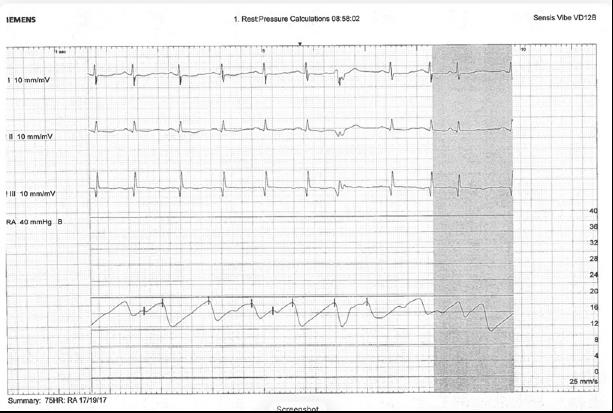
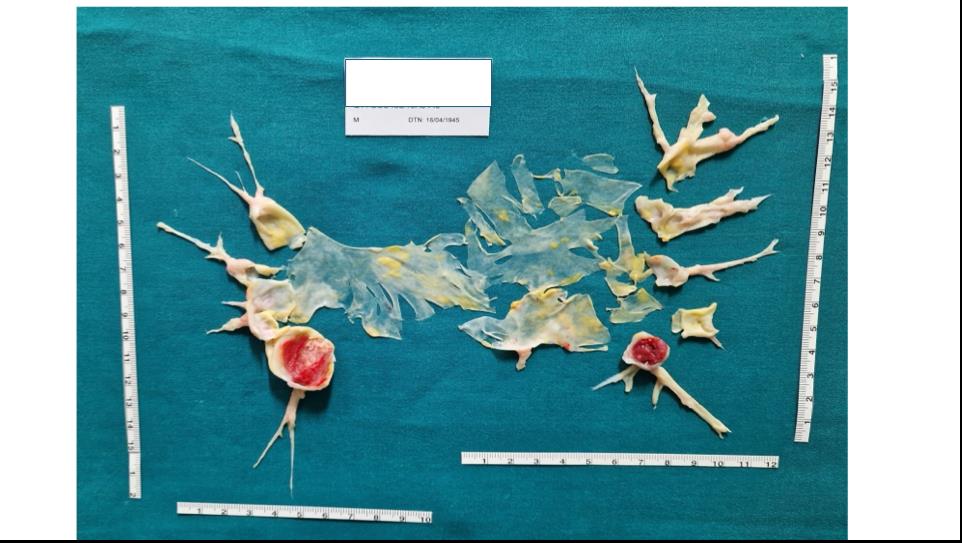
A 78 yo male presented to our Cardiology Department complaining of an increasing and severe dyspnoea. His anamnesis was relevant for a previous right myocardial infarction treated with percutaneous coronary angioplasty (PTCA) and a deep vein thrombosis treated with apixaban for 6 months with a recurrence after 4 years treated with rivaroxaban, still on board during our evaluation. The transthoracic echocardiogram showed a normal left ventricular systolic function, a D-shape appearance, with elevated filling pressures and a severe mitral regurgitation due to valve prolapse. On the right side a dilation of the right ventricle was accompanied by a severe tricuspid regurgitation with normal contractility parameters and high ventriculo-atrial gradient (sPAP 95 mmHg). The initial suspicion was a severe mitral regurgitation conditioning a secondary pulmonary hypertension (PH); the patient was then initiated with oral diuretic therapy and a trans-esophageal echocardiogram was then performed. After one month, diuretic therapy was effective in reducing mitral regurgitation alongside with left ventricular filling pressures, but, surprinsingly, estimated pulmonary pressures were still high (sPAP 95 mmHg). The patient underwent a high resolution CT scan and a contrast-CT chest scan which revealed no evidence of parenchymal disease, but multiple arterial filling defects. We then performed a right heart catheterization (RHC) via the internal giugular vein which revealed the following parameters: a medium pulmonary arterial pressure of 54 mmHg, a pulmonary artery wedge pressure (PAWP) of 17 mmHg, pulmonary vascular resistances of 6 wood units (WU), a central vein saturation of 56% and a reduced cardiac index (1.8 L/m2). No significant changes in saturation were found. Our parameters pointed towards the presence of a combined post capillary pulmonary hypertension with a severe reduction of cardiac index, which was coherent with the clinical and echocardiographic findings, but the PAWP waveform was not reflective of a correct catheter positioning (Fig.1) even after targeting the right lung zone 3 and arterial oxygen saturation was 96%. We then placed the Swan-Ganz catheter on the contralateral pulmonary branch thereby revealing a completely different curve with a PAWP of 7 mmHg (Fig.2) and a different diagnosis: a chronic thrombo-embolic pulmonary hypertension (CTEPH). The patient was then treated with a pulmonary thromboendoarterectomy surgery (Fig.3)