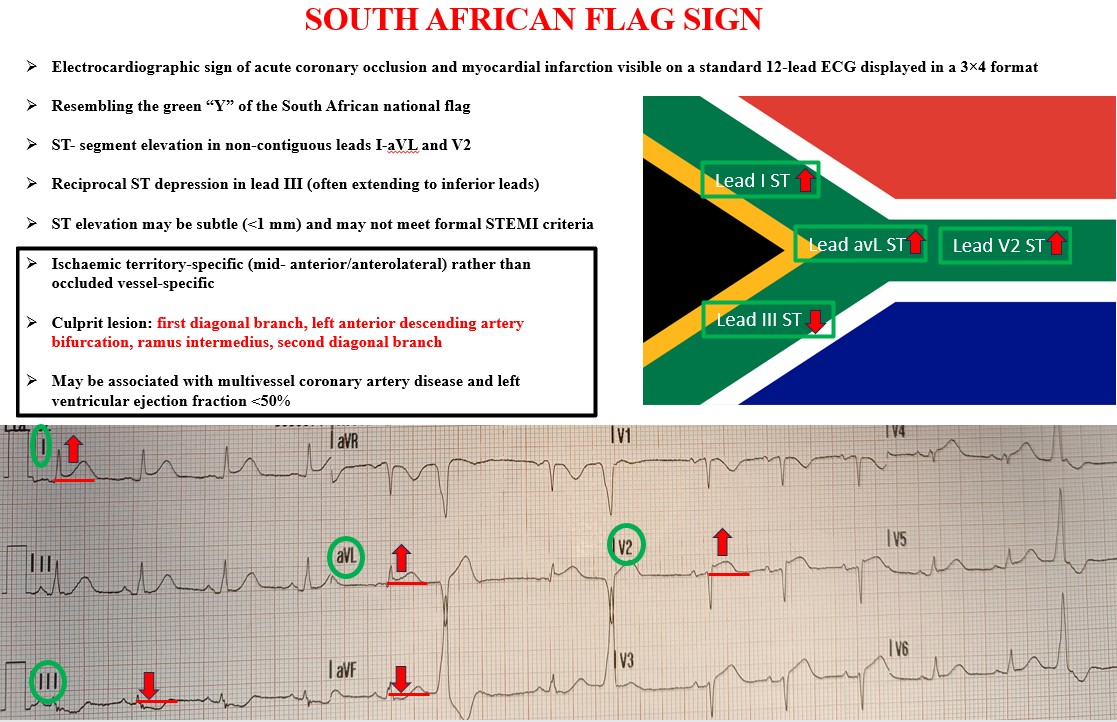
Background The South African flag sign (SAFS) is an electrocardiographic (ECG) pattern described by Littmann in 2015 for educational purposes. It is characterised by ST-segment elevation in leads I-aVL and the non-contiguous precordial lead V2, with reciprocal depression in lead III -avF, recreating the Y-shaped green element of the South African flag. Traditionally linked to first diagonal (D1) occlusion it is an increasingly recognized pattern of occlusion myocardial infarction, often not fulfilling classical ST- elevation myocardial infarction (STEMI) criteria. No specific review on this ECG sign has been conducted to date. Methods We systematically searched PubMed, MEDLINE, EMBASE, Scopus, Google scholar and grey literature, including reference list screening (2015–December 2025), to identify case reports and small series describing SAFS in acute coronary syndromes. Demographics,clinical, echocardiographic and ECG features, culprit vessel, left ventricular function, treatment and outcomes were extracted. Results Most cases were reported in 2025. We identified 21 reports describing 24 patients with SAFS, nearly all of whom underwent coronary angiography. Chest pain was universally present. Patients were diagnosed based on SAFS rather than classical STEMI criteria, reflecting the absence of guideline-specific recommendations.The culprit vessel was D1 or left anterior descending artery (LAD) bifurcation lesion in most cases, but ramus intermedius, multivessel disease, second diagonal branch of LAD, coronary aneurysms or no critical stenosis were also reported. Nearly all patients underwent urgent angioplasty with favourable in-hospital outcomes. Left ventricular ejection fraction was frequently <50%. No deaths occurred. Conclusions Available evidence indicates that SAFS is an under-recognised marker of acute transmural occlusion myocardial infarction, often not classified as STEMI because ST elevation can be subtle and appears in non-contiguous leads. The ECG pattern localises the ischaemic territory rather than a single culprit vessel and is consistent with transmural ischaemia arising from multiple potential occlusions rather than exclusively D1. Prompt identification of SAFS should trigger immediate coronary angiography and revascularisation. Given its diagnostic and prognostic relevance, this pattern merits formal inclusion in acute coronary syndrome guideline.