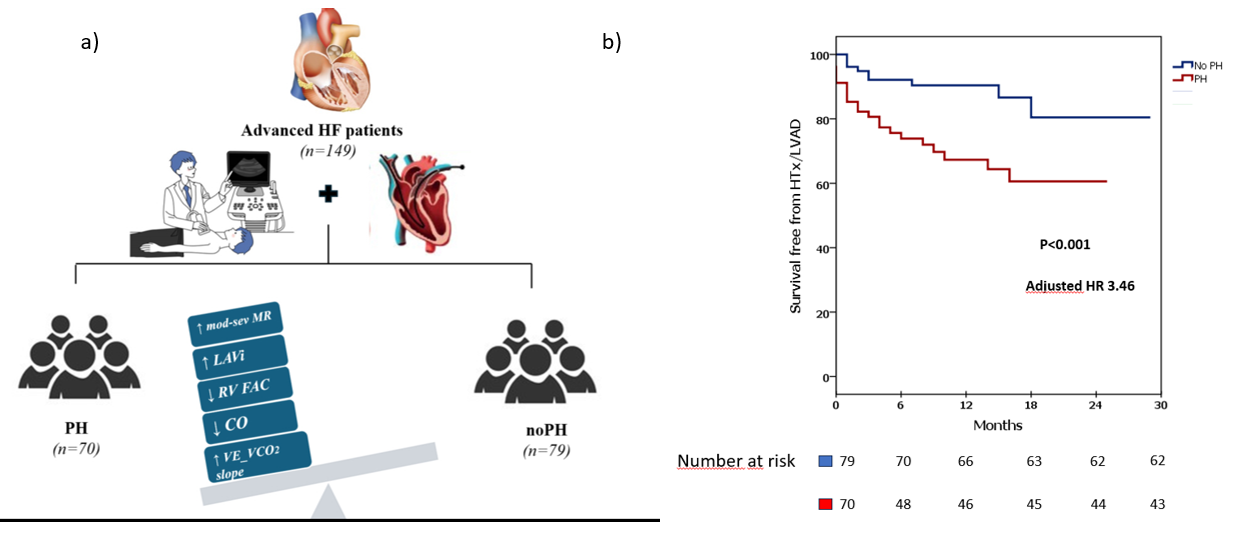
Background: Pulmonary hypertension (PH) complicates advanced heart failure (AdvHF) and may limit access to life-saving therapies such as heart transplantation (HTx). However, the independent prognostic value of PH in contemporary cohorts of patients with AdHF remains unclear. Methods: We prospectively enrolled ambulatory patients with at least one European Society of Cardiology (ESC) criterion for AdvHF referred to a tertiary centre for evaluation of advanced therapies. All underwent comprehensive clinical assessment, cardiopulmonary testing, echocardiography, and right heart catheterization (RHC); only patients with RHC and echocardiography within 24 hours were included. PH was defined according to the current ESC criteria for group 2 PH. The primary endpoint was a composite of all-cause death, left ventricular assist device implantation, or HTx. Results: Among 149 patients (mean age 53±12 years; 75% male; 36% ischemic heart disease; mean left ventricular ejection fraction 30±12%) 70 (47%) had PH at baseline. During follow-up, 44 patients (29.5%) experienced the primary endpoint, with a higher event rate in the PH group (38.6% vs 21.5%). In multivariable Cox analysis, PH remained the only independent predictor of the composite endpoint (HR 3.46, 95% CI 1.08–11.05; p=0.037). Conclusion: In ambulatory patients with AdvHF referred for advanced therapies, invasively confirmed PH is an independent prognostic determinant. Systematic assessment of PH should be integrated into risk stratification to optimize the timing of referral to advanced therapies.