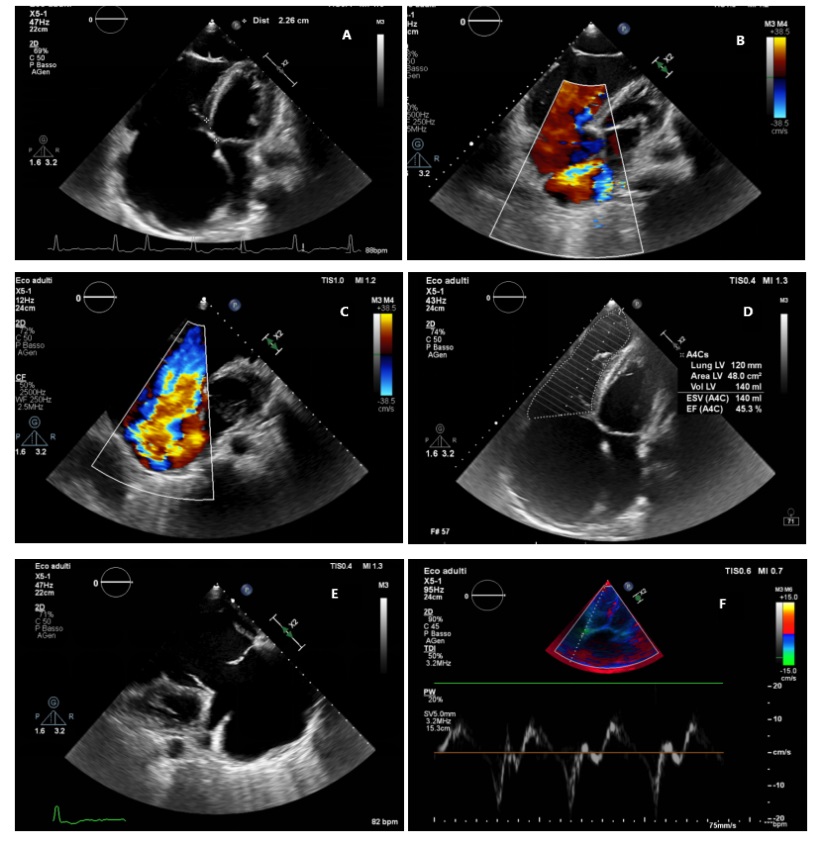
Introduction: Ebstein's anomaly is a rare congenital cardiac disease, defined as the significant apical displacement of the part of the tricuspid valve due to inadequate delaminization of the tricuspid valve tissue. This condition causes significant tricuspid regurgitation and reduction of the functional right ventricle and right ventricular dilatation. We present a case of right heart failure in adult patient with Ebstein's anomaly and a cor triatriatrium as additional defect. The case: A 60 man was admitted to our hospital with right heart failure. The cardiovascular examination showed jugular venous distension, pitting edema, and systolic murmurs 3/6. The patient was not cyanotic and his vital signs were stable. His ECG showed atrial fibrillation, RBBB and right ventricular hypertrophy. A marked cardiomegaly on chest x-ray film was revealed (Figure 1). Observation of two-dimensional echo showed severe RV and RA dilatation (RVD1 73,8 mm; 84 cm2, Figure 2, Panel A); his RV fractional area change [RVFAC] was 45 % (Figure 2, panel D), but he had a normal and tricuspid annular plane systolic excursion (TAPSE 18 mm). He had also a RV atrialization, with apical dislocation of the tricuspid septal flap as a mild Ebstein anomaly, with a distance from the AV junction of approximatelly 23 mm (15 mm/m2) (Figure 2, panel A) and lack of coaptation between the valve leaflets and consequent massive tricuspidal insufficiency (Figure 2, panel C). Transthoracic echocardiography (TTE) revealed also a non-obsructive cor triatriatum dexter as additional defects (Figure 2, Panel B). Coronary angiography and cardiac catheterization were planned to evaluate pulmonary pressures and estabilish the following therapeutic strateg Discussion: Echocardiography is diagnostic in most patients and demonstrates apical displacement of the septal leaflet and variable tethering of leaflet tissue to the right ventricular myocardium.The therapeutic strategy may be based on medical management in its mild asymptomatic forms up to surgical interventions that include tricuspid valvuloplasty, palliative surgery, valve replacement or cardiac transplantation. Operative intervention is considered for exertional symptoms, progressive right ventricular enlargement, or right ventricular dysfunction. Tricuspid valve cone repair is the preferred surgical approach. Tricuspid valve replacement and bidirectional cavopulmonary shunt also are considered in patients with advanced disease.