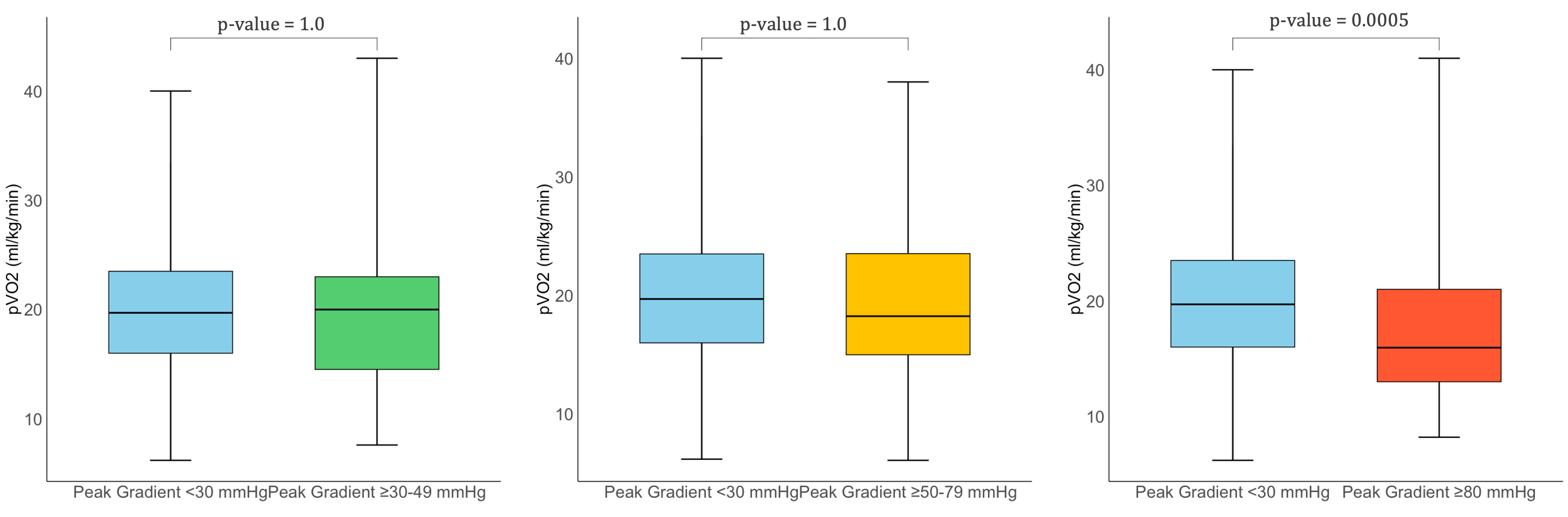
Background: Hypertrophic cardiomyopathy (HCM) is a complex disease in which left ventricular outflow tract (LVOT) obstruction influences both functional capacity and clinical outcomes. However, the clinical relevance of varying obstruction severity remains debated. Objectives: To evaluate the relationship between LVOT gradient severity and both exercise performance and long-term prognosis in HCM using combined cardiopulmonary exercise testing and stress echocardiography (TTE-CPET). Methods: We retrospectively analyzed 388 HCM patients undergoing TTE-CPET, stratified into four groups based on peak LVOT gradient: <30 mmHg, 30–49 mmHg, 50–79 mmHg, and ≥80 mmHg. Clinical, echocardiographic, and CPET data were compared. The primary outcome was a composite of NYHA class worsening, heart failure hospitalization, new-onset atrial fibrillation, or progression to end-stage HCM, assessed over a median follow-up of 7.4 years. Results: Only patients with severe obstruction (≥80 mmHg, n=82) showed significantly lower peak VO₂ (15.9 vs. 19.7 ml/kg/min, p=0.003), higher pulmonary pressures, more advanced diastolic dysfunction, and greater symptom burden. They also had a higher incidence of adverse events (50.0% vs. 31.6%, p=0.011) and worse event-free survival (log-rank p=0.011). A peak gradient ≥80 mmHg independently predicted adverse outcomes (HR: 1.87; p=0.009), even after adjustment. Patients with intermediate gradients (30–79 mmHg) had generally preserved outcomes, though some exhibited early structural or functional changes Conclusions: Severe dynamic LVOT obstruction identifies a high-risk HCM subgroup with impaired exercise capacity and poor prognosis. Intermediate gradients may still warrant close monitoring. TTE-CPET offers critical insight for risk stratification and early intervention.