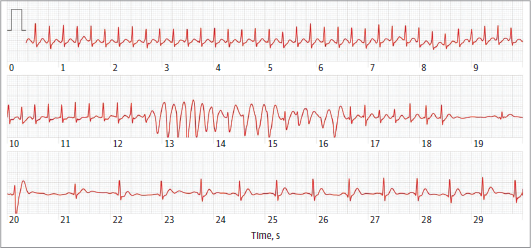
Case Presentation A young adult patient was referred to our Arrhythmic Unit for palpitations.The patient's anamnesis revealed no previous arrhythmic episodes or family history of SCD. The physical examination results were unremarkable. The patient’s smartwatch recorded a narrow QRS regular tachycardia triggering a nonsustained phase of wide complex irregular tachycardia; finally, the tachycardia again assumes a wide complex configuration until spontaneous termination occurs some beats later. The interpretation of the “narrow-wide-narrow” QRS complex tachycardia was not univocal: polymorphic VT, aberrant conduction, or artifact. The wide complex irregular tachycardia started with an end-diastolic wide QRS complex. The ventricular rate slightly increases as the tachycardia begins.There were at least fusion complexes and the absence of compensatory pause at the end of wide complex irregular tachycardia. Moreover, the narrow QRS tachycardia reappears with the same starting cycle length. The patient underwent a treadmill stress test, which was negative for arrhythmias. The electrophysiology study revealed a slow-fast AVNRT with a cycle length of 250ms; no accessory pathway or aberrant conduction was shown. The programmed ventricular stimulation was negative for the inducibility of any VTs.The radiofrequency ablation of the slow pathway was successfully performed, and the patient was discharged. Discussion The diffusion of smartwatches is rapidly increasing. It has been reported that the diagnostic accuracy of smartwatches with a photoplethysmography is high in detecting AF. The association of dual AV node physiology, AVNRT, and idiopathic ventricular tachycardia has been described. However, AVNRT degenerating into polymorphic VT is rare; simultaneous VT and SVT, which coexist at a similar rate without affecting the ventricular focus discharge, is just as rare. The presence of transition from narrow complex to wide-complex tachycardia with different cycle lengths and different QRS morphology excluded the possibility of AVNRT conducted over a bystander accessory pathway. There start of narrow QRS tachycardia with the same cycle length as that before wide complex tachycardia excluded the hypothesis of VT. The electrophysiology study confirmed the diagnosis of AVNRT. Finally, we considered the phase of wide irregular QRS tachycardia as an artifact. The present case suggests that attention should be paid to the ECG findings of smartwatches.