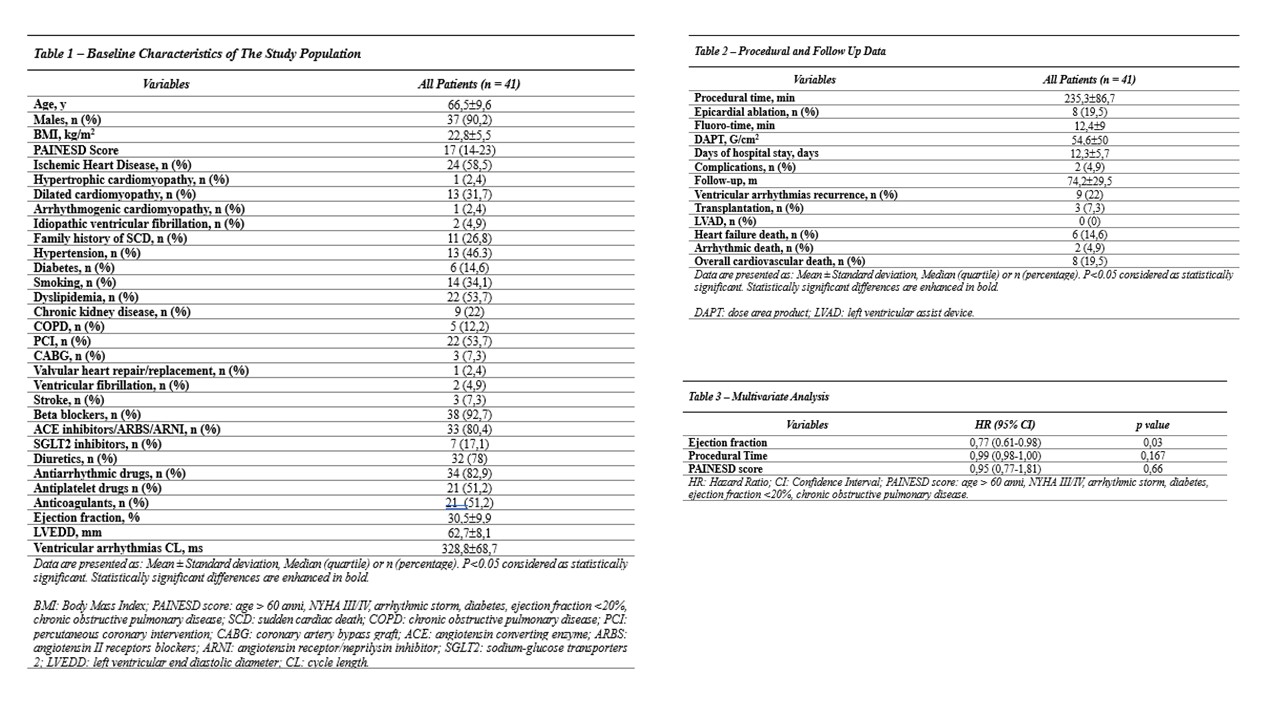
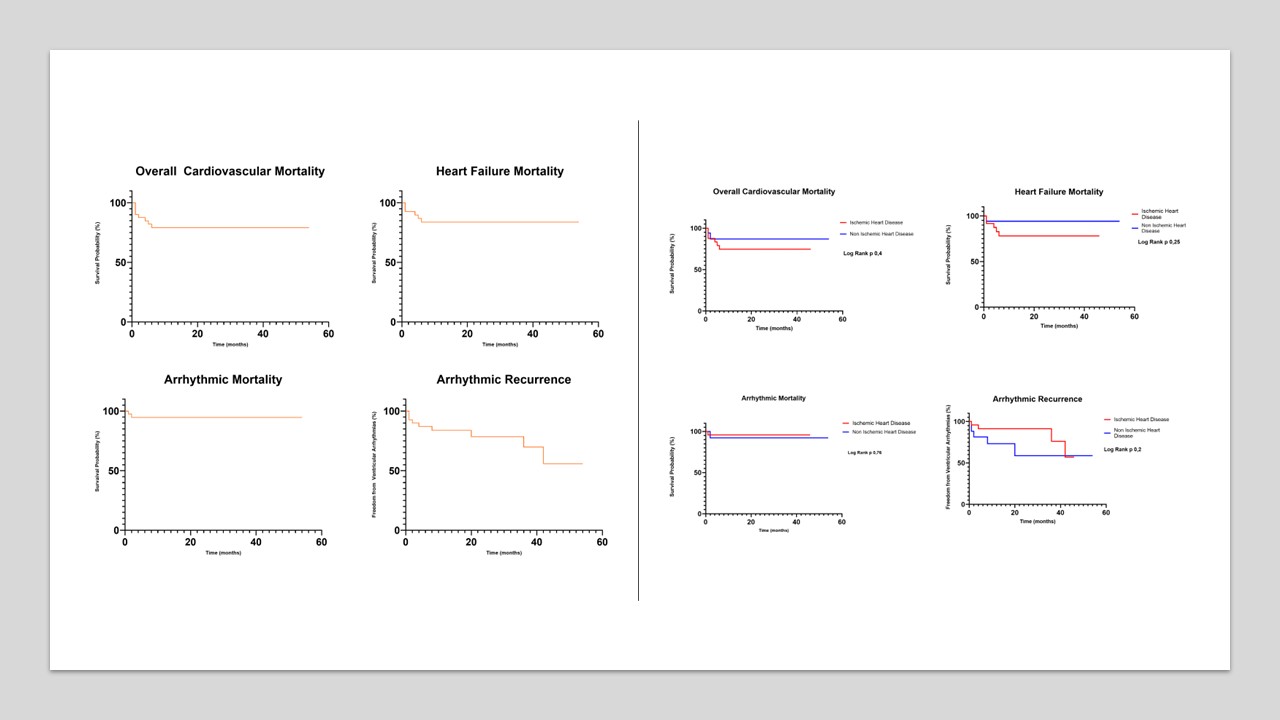
Background Catheter ablation is a treatment option for sustained ventricular tachycardias (VTs) that are refractory to pharmacological treatment; however, patients with fast VT and electrical storm (ES) are at risk for cardiogenic shock. Extracorporeal membranes oxygenation (ECMO) has been proposed as a useful tool for managing these procedures and facilitate the accurate mapping and ablation of unstable VAs. P urpose The aim of this study is to assess the clinical outcome of cardiopulmonary support during a long-term follow-up. Methods In this retrospective study, we analyzed patients who underwent ventricular arrhythmias catheter ablation supported by ECMO, under deep sedation, in our center, between 2016 and 2024. The primary endpoint was overall survival from cardiovascular death. The secondary endpoint was death due to heart failure or arrhythmias and arrhythmic recurrences. Survival analysis was performed using Kaplan-Meier curves and Cox proportional hazard model as multivariate analysis. Then, mortality was stratified according to the type of underlying heart disease. Results A total of 41 patients (mean age 66,5±9,6 years; 90.2% males) were included in this study. Baseline clinical characteristics are reported in fig.1. 58,5% of patients were affected by ischemic heart disease; medium PAINESD score was 17 (14-23). Procedural data are shown in fig.1: mean procedural time was 235,3±86,7 minutes, fluoro-time was 12,4±9 minutes and dose area product was 54,6±50 G/cm 2 . After a median follow-up of 74.2 ± 29.5 months, overall cardiovascular mortality was 19.5%, (fig.1 and fig.2). Concerning the secondary outcome, 6 (14,6%) died due to heart failure, 2 (4,9%) because of arrhythmic death. 32 patients (78%) were free from arrhythmic recurrences. Three patients underwent heart transplantation. No differences were observed between ischemic and non-ischemic heart disease regarding mortality incidence (fig.2). After univariate analysis, only ejection fraction remained a predictor of mortality in multivariate analysis (fig.1). Two complications were documented: one femoral artery stenosis and one hemorrhagic shock. Conclusion ECMO is a safe and effective tool to support ventricular arrhythmia ablations, showing good procedural and long-term clinical outcomes. There are no significant differences in mortality considering the type of underlying heart disease. Higher ejection fraction is a protective factor from mortality.