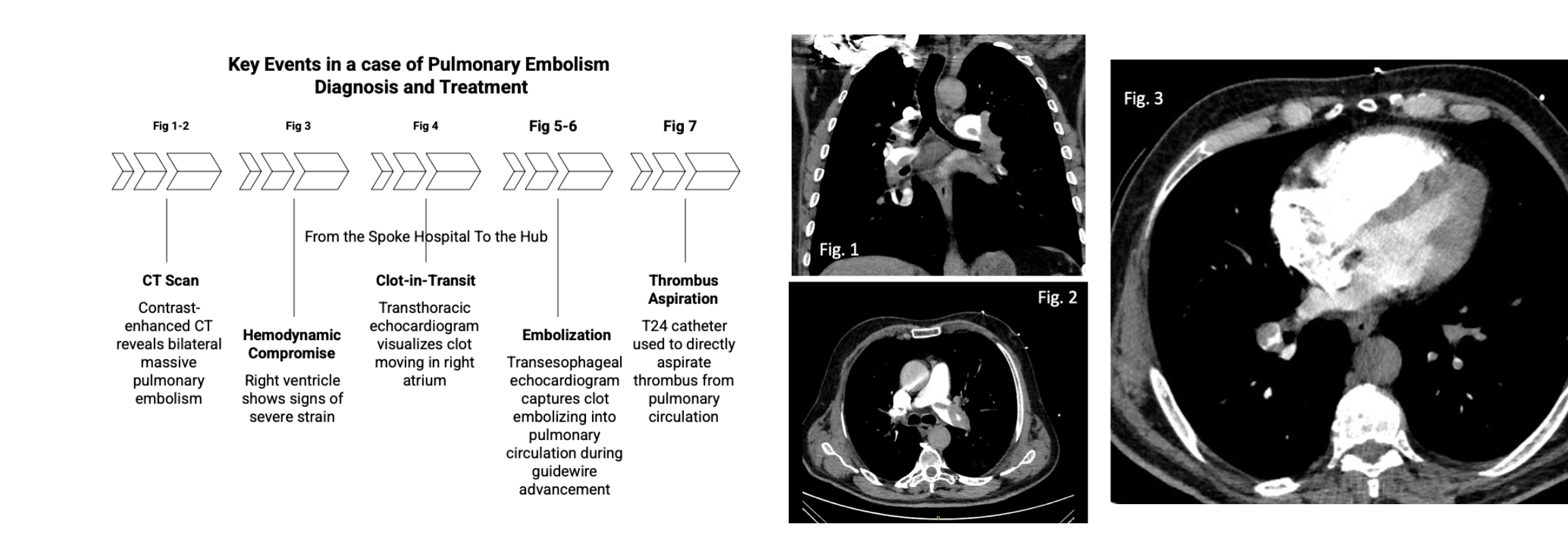
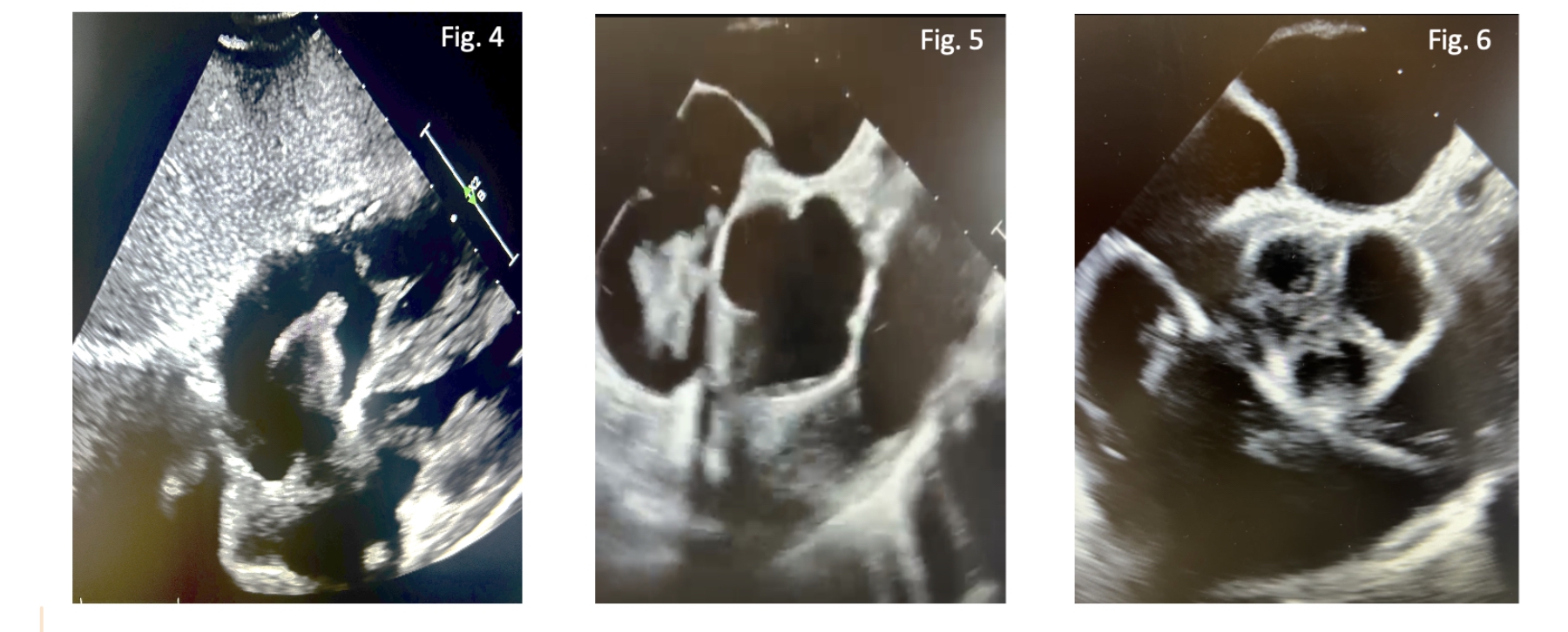
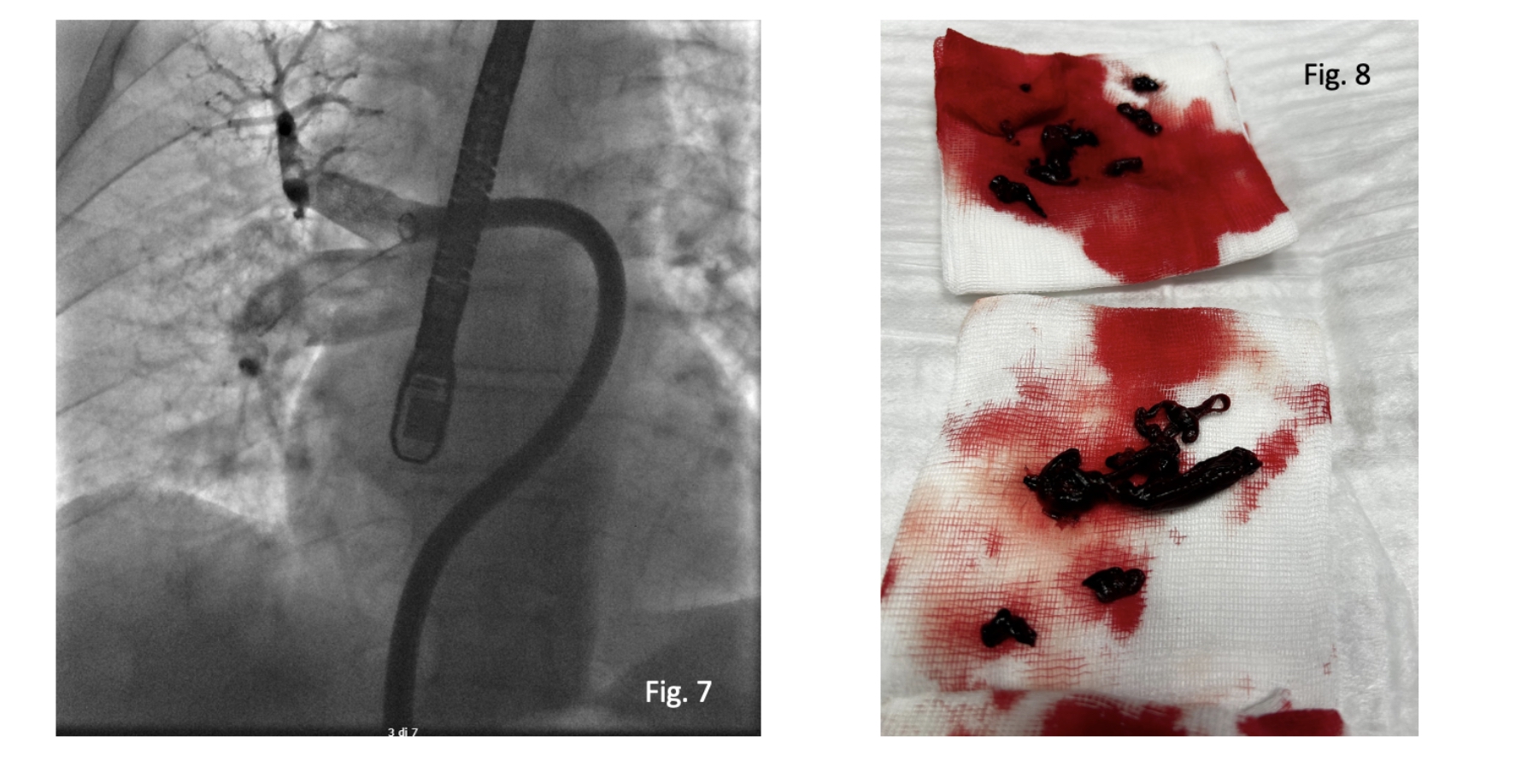
A 75-year-old male presented to the emergency department with acute, progressively worsening dyspnea associated with syncopal episode. Initial presentation included a BP 125/65 mmHg, a HR <110 bpm, and SO2 97%. Arterial blood gas analysis revealed normal pH, mild hypocapnia, and elevated plasma lactate levels. Troponin Hs 53 ng/L, NT-proBNP 799 pg/mL, and D-dimer >20,000 ng/mL. Computed tomography (CT) of the chest demonstrated a filling defect in the common arterial trunk and a "saddle" thrombus extending into both main pulmonary arteries. TTE revealed reduced right ventricular (RV) function and dilated RV dimensions with a D-shaped septum. A mobile, serpiginous image was noted in the right atrium, extending to the tricuspid valve plane, consistent with a clot-in-transit (Fig 1-3) The (PESI) score was 115, indicating a high mortality risk (8.9%). Given the size and mobility of the clot-in-transit in intermediate-high risk pulmonary embolism the pulmonary embolism response team (PERT) decided to perform mechanical thrombectomy using the FlowTriever® system (Inari Medical) due to the high risk of clinical deterioration caused by recurrent embolization. While initially intended for the treatment of pulmonary embolism, it can also be used off-label to treat thrombi in other locations, such as the cardiac atria or ventricles. The procedure was planned following a multidisciplinary discussion with PERT and was performed after oro-tracheal intubation. The passage of the Triever24 was always monitored by transesophageal echocardiography in order to identify the thrombus and guide the thrombus aspiration During this maneuver transesophageal echocardiographic monitoring revealed the embolization of the thrombotic material through the right heart chambers with the need of a rapid change of strategy (Fig 4-6) The patient's hemodynamic condition rapidly deteriorated into overt shock, necessitating the infusion of high-dose norepinephrine and dobutamine. Immediately the aspiration catheters (Triever24 and Triever20) were advanced to the pulmonary thrombosis with removal of multiple thrombi and rapid improvement of hypotension (Fig 7-8) Arterial blood gas analysis at the conclusion of the procedure showed a pH of 7.1, lactate of 1.7 mmol/L, PCO2 of 68 mmHg ETT performed 4 days later revealed a reduction in RV dimensions and an improvement in RV function. Tricuspid regurgitation (TR) improved from severe to mild. The patient was discharged from the ICU on Day 5.