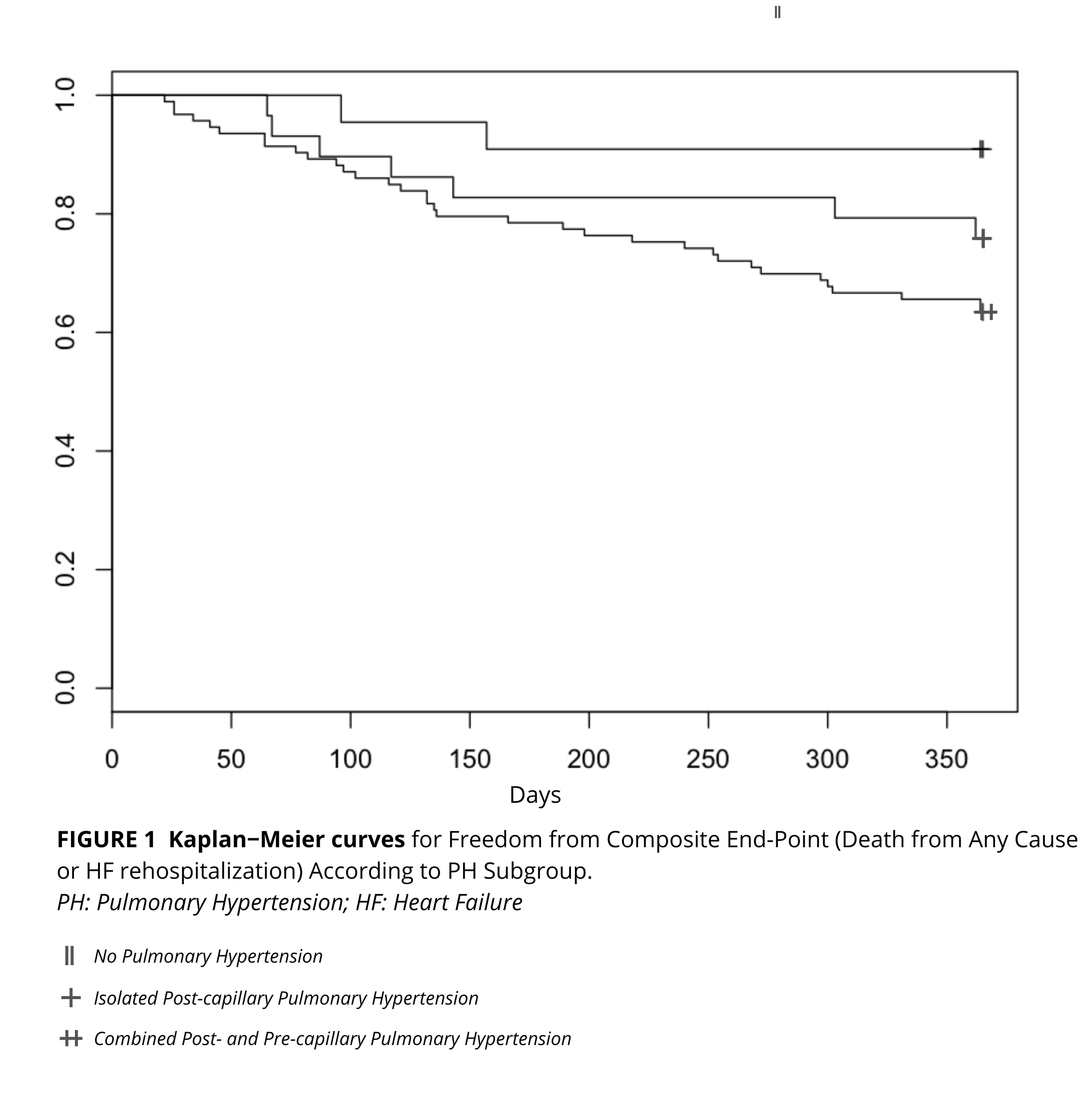
Background: Functional mitral regurgitation (FMR) is a common complication in patients with heart failure with reduced ejection fraction (HFrEF), often accompanied by pulmonary hypertension (PH), which worsens prognosis. Transcatheter edge-to-edge mitral valve repair (M-TEER) has demonstrated efficacy in improving outcomes in FMR; however, the influence of PH, including its subtypes, on these outcomes remains poorly investigated. This study investigates 1-year outcomes of M-TEER in HFrEF patients with FMR and PH, focusing on PH subtypes. Methods: We conducted a multicenter, retrospective analysis of consecutive HFrEF patients with moderate-to-severe FMR who underwent M-TEER. Baseline data were collected, including echocardiographic, hemodynamic, and clinical characteristics. PH was diagnosed and classified using right heart catheterization (RHC) into isolated post-capillary PH (Ipc-PH) and combined post- and pre-capillary PH (Cpc-PH). Procedural outcomes and 1-year clinical results, including mortality and heart failure (HF) rehospitalizations, were evaluated. Results: Among the 144 patients included, 80% had PH, with 57% classified as Cpc-PH and 23% as Ipc-PH. M-TEER showed high procedural success (92%) and significant improvements in functional status. At 1-year follow-up, patients with PH exhibited worse outcomes compared to those without PH, with HF rehospitalization rates of 32% vs. 7% (p = 0.016) and a composite endpoint (death or HF rehospitalization) of 34% vs. 11% (p = 0.025). Cpc-PH was independently associated with poorer outcomes, including HF rehospitalization (adjusted HR 8.2, 95% CI: 1.1–62.6; p = 0.037) and the composite endpoint of death or HF rehospitalization (adjusted HR 4.3, 95% CI: 1.02–18.4; p = 0.046). Conclusion: M-TEER is an effective intervention for FMR in HFrEF patients, but PH, particularly Cpc-PH, significantly impacts prognosis. Pre-procedural evaluation of PH subtypes using RHC is essential for risk stratification and therapeutic planning.