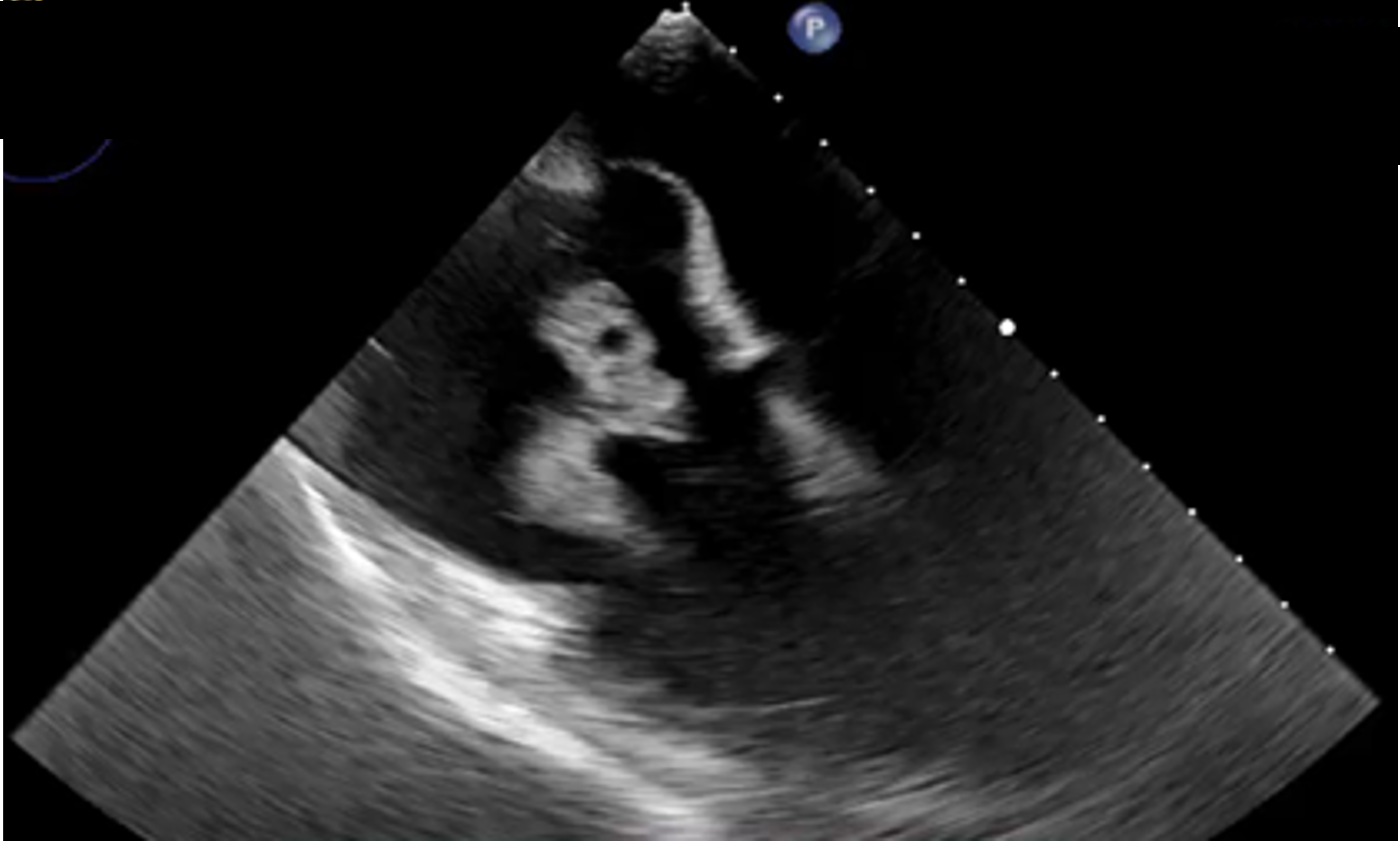
A 45-year-old male patient with a history of intravenous drug use, chronic anemia, and erosive gastritis presented to the emergency department with fever and dyspnea. Laboratory tests revealed severe anemia (Hb 6 g/dL), marked leukocytosis, elevated d-dimer (23.57 mg/L), C-reactive protein (188 mg/L), procalcitonin (9.73 ng/mL), and increased lactic acid levels. A chest computed tomography scan excluded acute thromboembolism but revealed multifocal ground-glass and nodular opacities with internal cavitation, suggestive of septic emboli [Figure 1]. Transthoracic and transesophageal echocardiography identified two large, mobile vegetations on the tricuspid valve’s septal leaflet, measuring 38 × 16 mm and 27 × 8 mm and a severe tricuspid regurgitation [Figure 2]. Blood cultures were obtained, and based on the Duke criteria, a diagnosis of infective endocarditis was made. Multiple red blood cell transfusions were performed and empiric antibiotic therapy was promptly initiated. Due to the patient’s critical condition, the heart team deemed him a poor candidate for surgical tricuspid valve replacement. Blood cultures subsequently tested positive for methicillin-sensitive Staphylococcus aureus (MSSA) and Enterococcus faecalis. The antimicrobial regimen was adjusted accordingly. However, despite appropriate antibiotic therapy, the patient’s clinical and hemodynamic status worsened. Non-invasive ventilation with bi-level positive airway pressure and norepinephrine support became necessary. Given the rationale of reducing bacterial burden, the heart team opted for a minimally invasive approach: the percutaneous mechanical vegetation debulking using the AngioVac system [Figure 3]. Following the intervention, the patient completed antibiotic therapy without further episodes of fever or septic lung embolizations and later was discharged in stable condition. Infective endocarditis (IE) is a multisystemic disease primarily affecting the heart valves. Large vegetations, peripheral embolic phenomena, and persistent bacteremia are typical indications for cardiac surgery. However, while surgery remains the first-line treatment for infective endocarditis unresponsive to antibiotics, the AngioVac system offers a minimally invasive alternative, particularly in critically ill and high-risk surgical candidates. The case report highlights the successful results of AngioVac system in decreasing infectious burden by removing vegetations and limiting further septic embolizations.