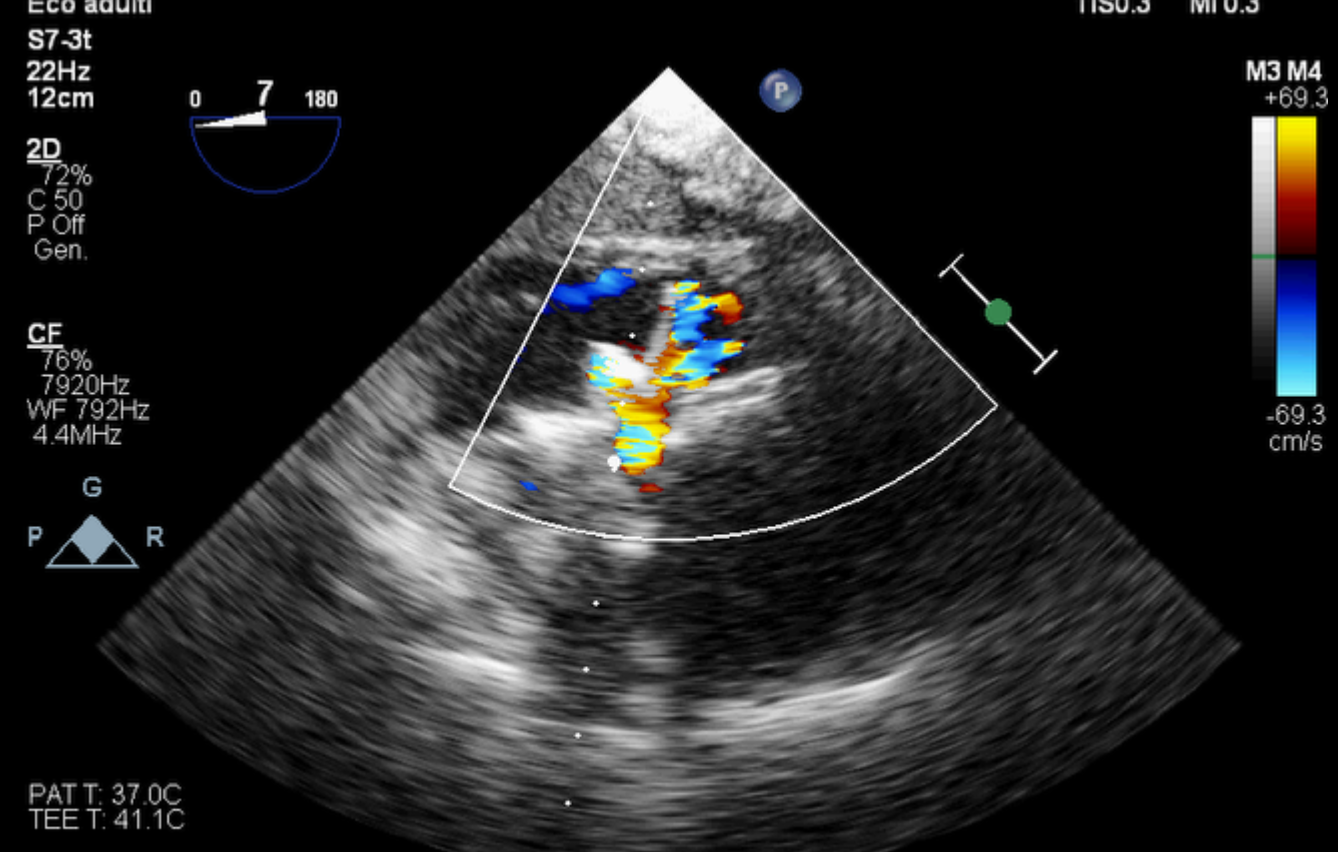
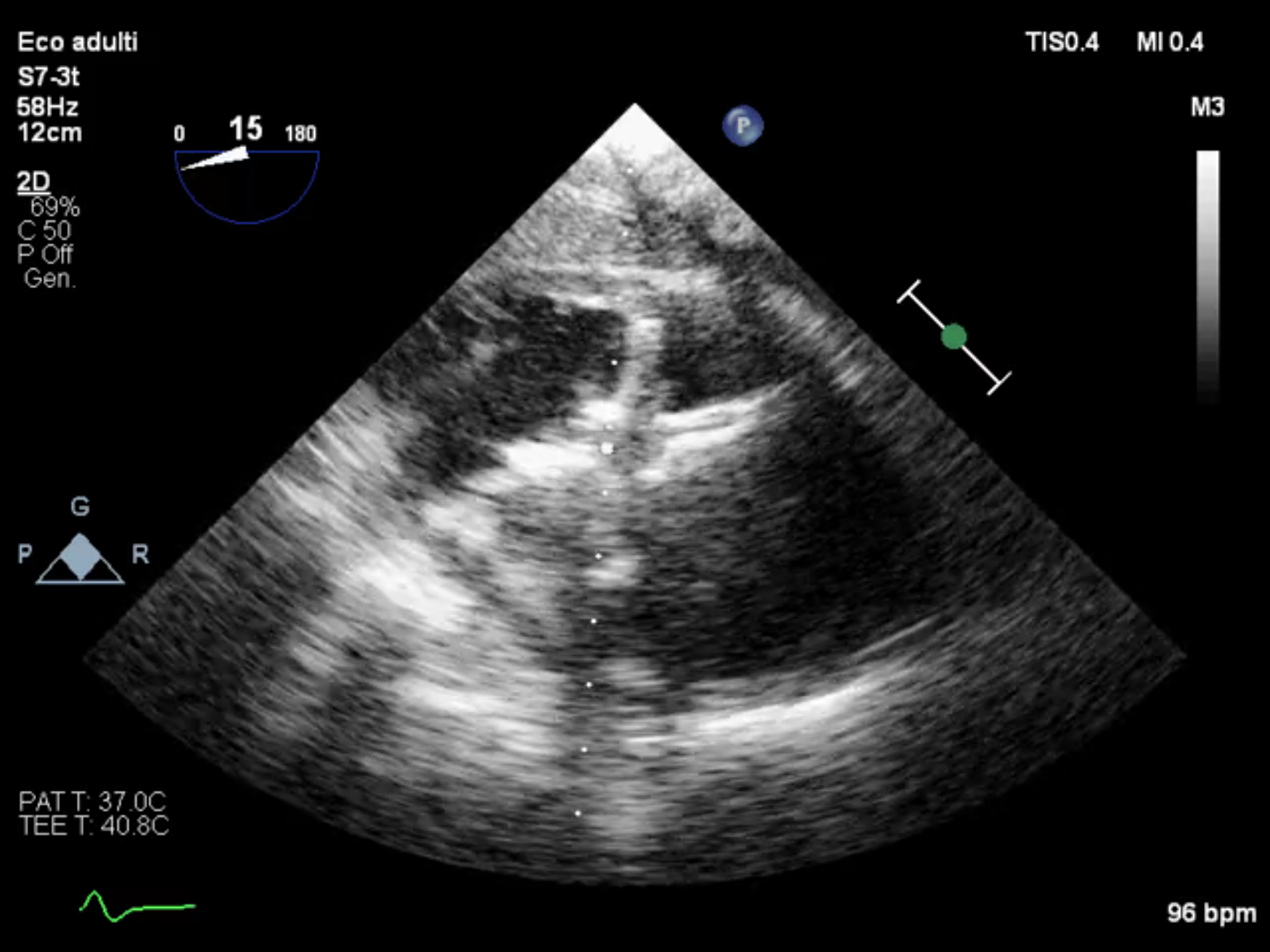
Case description: A 57-year-old patient with a history of systemic hypertension, smoking, and type 2 diabetes mellitus presented to the emergency department with chest pain of approximately 2 days' duration. ECG showed ST-segment elevation in the anterior leads and elevated cardiac necrosis markers. Transthoracic echocardiography revealed moderately reduced global systolic function (EF 45%), akinesis of the apex, septum, and inferior wall, with evidence of an interventricular septal defect located at the posterior septum with left to right shunt. Coronary angiography demonstrated a non-revascularizable thrombotic occlusion of the left anterior descending artery and chronic occlusion of the right coronary artery. Due to hemodynamic instability, the patient was supported with IABP, norepinephrine, intubated, and ultrafiltered. During the hospitalization, the patient developed a K. pneumoniae pneumonia, which subsequently resolved. Once the clinical condition stabilized, a multidisciplinary team decided to proceed with a percutaneous closure of the ventricular septal defect (VSD) due to the patient's extreme frailty and high surgical risk. The procedure was performed under angiographic and transesophageal echocardiographic guidance, using a 26 mm Amplatzer septal occluder, with residual intra- and peri-prosthetic shunts. The patient subsequently stabilized. Discussion: Ventricular septal rupture is a rare (0.25% of cases) mechanical complication associated with acute myocardial infarction, characterized by high mortality. It is characterized by the acute onset of a left-to-right shunt, which most often manifests as cardiogenic shock with low output and pulmonary overflow. While current guidelines favor a surgical approach, most studies comparing the two techniques have a selection bias, as patients receiving the percutaneous approach were frailer and had contraindications to cardiac surgery. Factors favoring percutaneous closure include defect size (<24 mm), single defect, adequate margins, and distance from the valves. Regarding the timing of the intervention, some studies have shown lower mortality if it can be postponed for at least seven days to allow for tissue reorganization. In these patients, if hemodynamics permit, vasodilators should be preferred as reducing afterload reduces the intracardiac shunt. In cases where mechanical support is required, IABP is the main application.