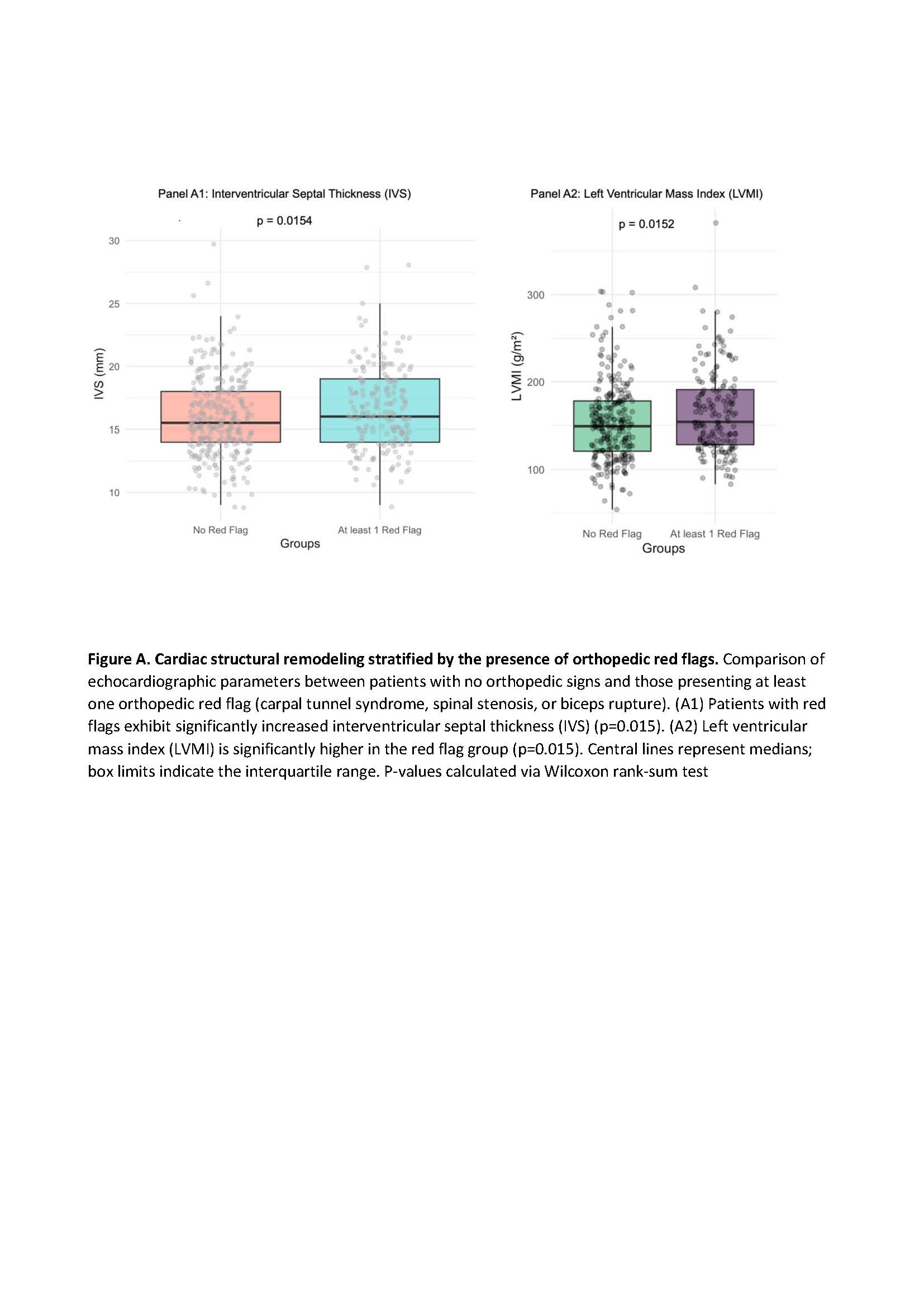
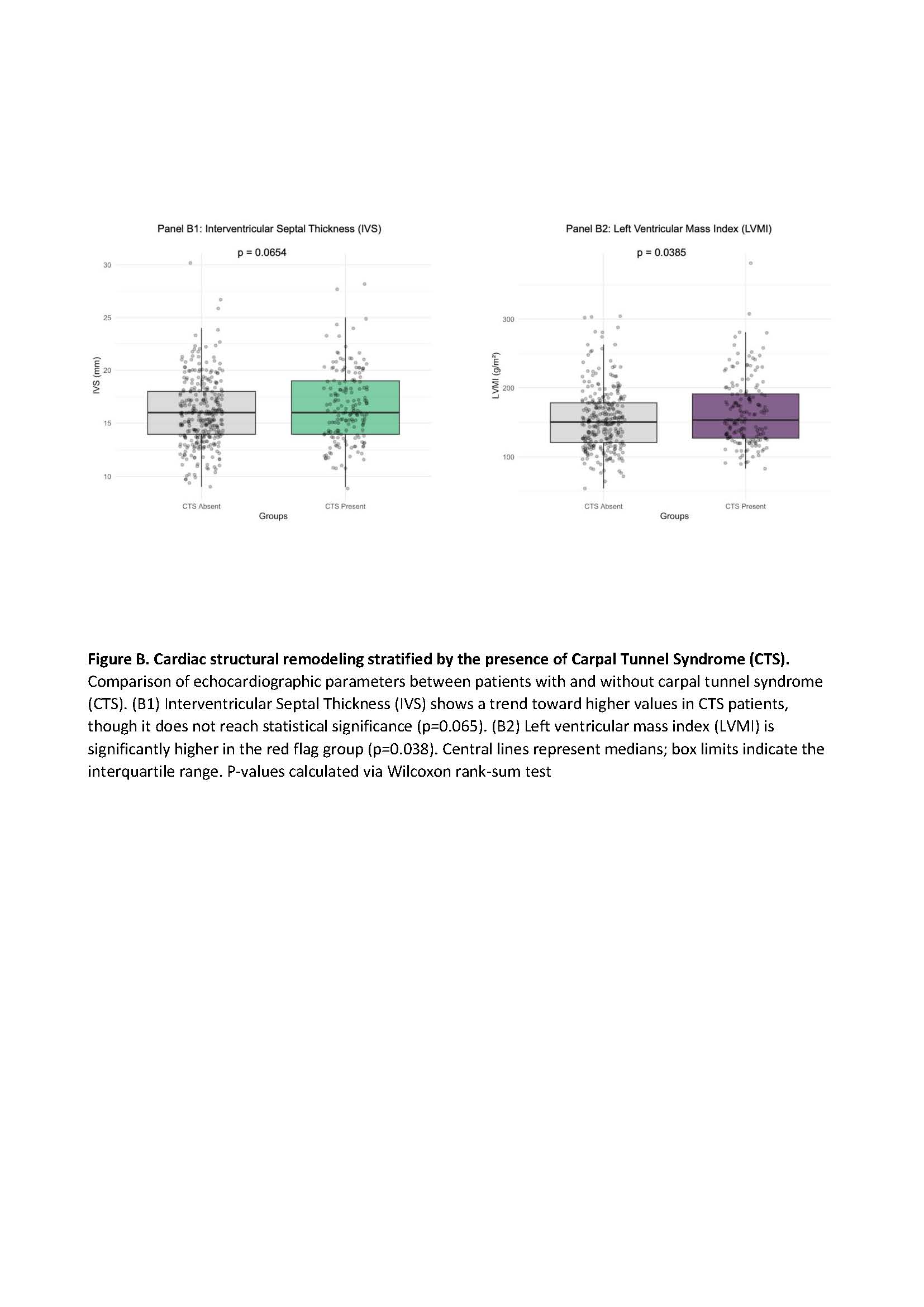
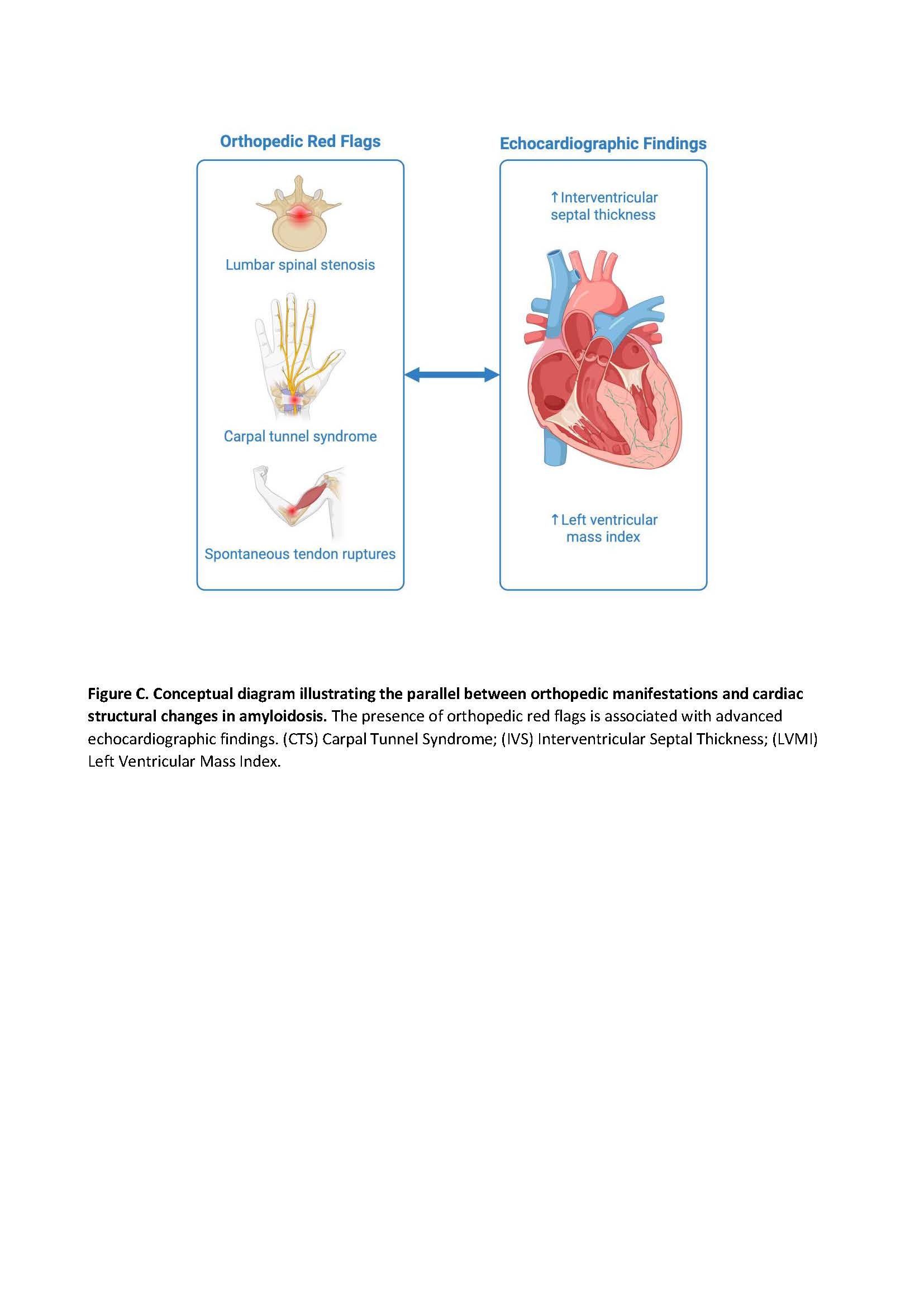
Background: Cardiac amyloidosis (CA) is a systemic infiltrative disease often associated with musculoskeletal manifestations. Orthopedic "red flags" include carpal tunnel syndrome (CTS), lumbar spinal stenosis, and spontaneous rupture of the distal biceps tendon. While their role in early suspicion is established, the association between the presence of these orthopedic signs and the severity of cardiac structural involvement at the time of diagnosis remains under investigation. Aim: The aim of this study was to evaluate the correlation between the presence of orthopedic red flags and echocardiographic markers, specifically interventricular septal thickness (IVS) and left ventricular mass index (LVMI). Methods: We retrospectively analyzed data from patients referred to our tertiary center for the diagnostic work-up and management of CA from 2018 to 2025. Medical history was collected and echocardiography was performed. We performed two analyses: (A) Comparing patients with "at least one orthopedic red flag" vs. "no red flags"; and (B) Comparing patients with "CTS" vs. "No CTS". Continuous variables were compared using the Wilcoxon rank-sum test. Results: We enrolled 551 patients (80% male, mean age 77 years) with confirmed ATTR (n=425), AL (n=122), ATTR+AL (n=2), and AA amyloidosis (n=2). The prevalence of orthopedic red flags was CTS in 170 patients (30.85%), distal biceps tendon rupture in 25 (4.54%), and spinal canal stenosis in 37 (6.72%). In Analysis A, in patients with at least one orthopedic manifestation, IVS was significantly higher in the red flag group (median: 16 [IQR: 5] vs. 15.5 [IQR: 4], p = 0.015), as was LVMI (median: 154 [IQR: 62.5] vs. 149 [IQR: 57], p = 0.015) compared to those without red flags. In Analysis B, patients with a history of CTS exhibited a significantly higher LVMI (median: 157 [IQR: 62.8] vs. 150 [IQR: 57], p = 0.038). The difference in IVS for the CTS group showed a trend toward increased thickness but did not reach statistical significance (median: 16 [IQR: 5] vs. 16 [IQR: 4], p = 0.065). Conclusions: Our data suggest that orthopedic red flags are not merely early warning signs but are associated with a more advanced cardiac phenotype. Patients with a history of orthopedic involvement present with significantly greater IVS and LVMI. This correlation implies that the systemic burden of amyloid deposition in the musculoskeletal system may parallel the magnitude of myocardial infiltration (Figure C).