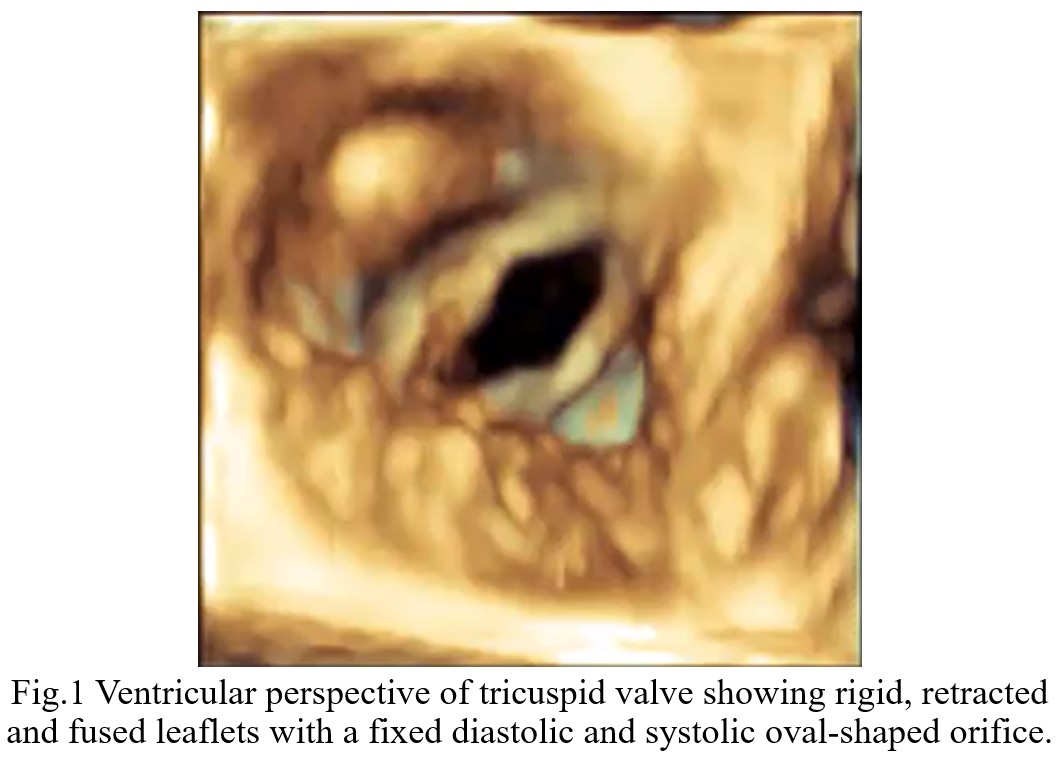
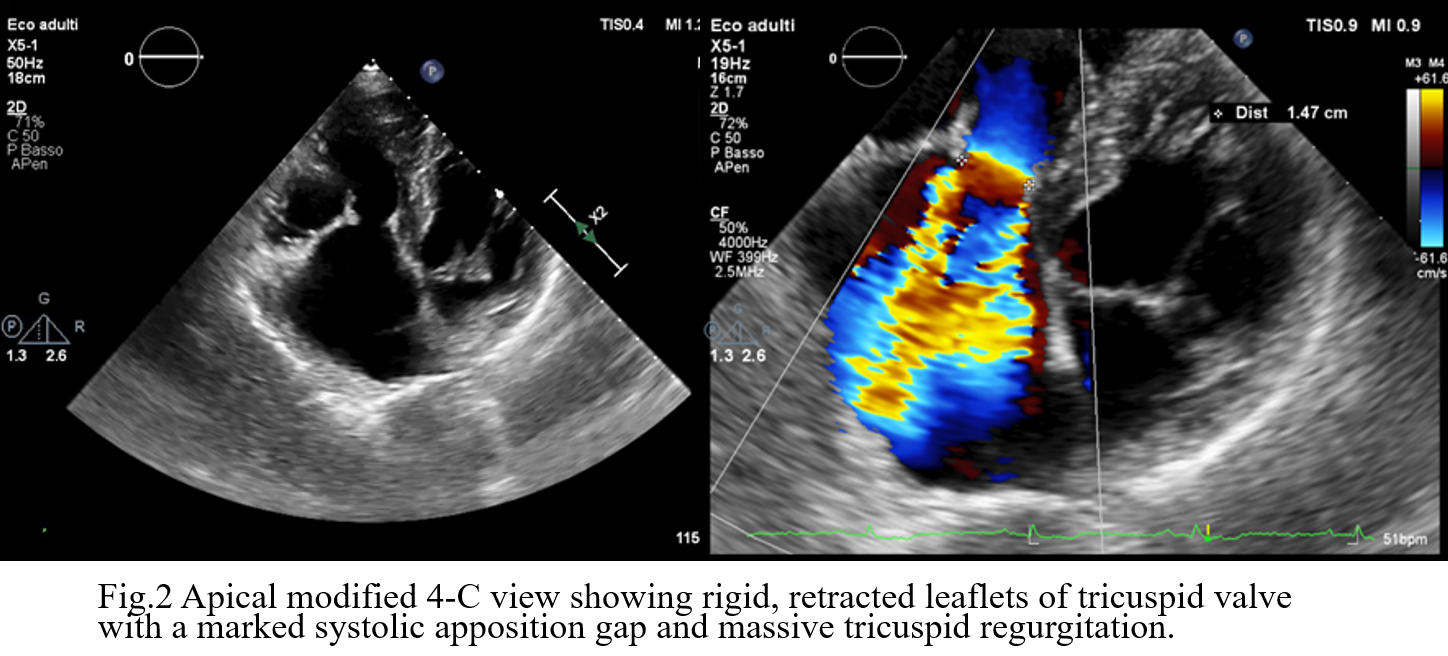
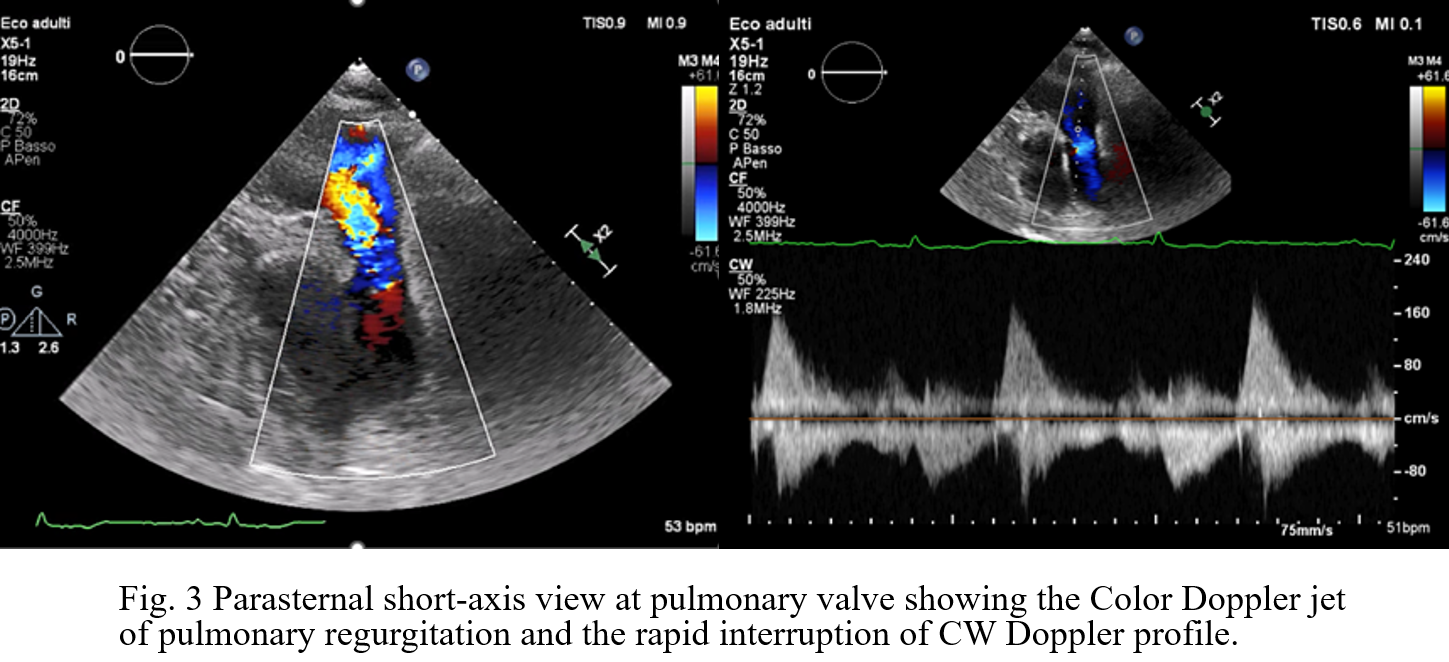
Background: Carcinoid Heart Disease (CHD) is a rare but ominous complication of neuroendocrine tumors (NETs), characterized by fibrotic plaque deposition on endocardial surfaces. While tricuspid valve involvement is well-documented, the pulmonary valve is often overlooked despite its significant impact on right ventricular (RV) hemodynamics. Case Presentation: A 73-year-old male with an ileal NET and liver/peritoneal metastases, stable under lanreotide acetate for four years, presented with progressive dyspnea and peripheral edema. Initial transthoracic echocardiography (TTE) and cardiac MRI identified severe tricuspid regurgitation (TR) and significant right heart dilation. The patient was referred to our Department to explore the feasibility of transcatheter tricuspid intervention. Advanced Imaging Findings: Comprehensive TTE and transesophageal echocardiography (TEE) confirmed RV dilation (RVD1 49 mm, RVOT 44 mm) with preserved systolic function (TAPSE 22 mm, FAC 48%). The tricuspid valve exhibited classic CHD features: fibrotic, retracted, and rigid leaflets with commissural fusion. 3D echocardiography showed a fixed, oval-shaped orifice (1.6 cm²) that remained immobile throughout the cardiac cycle due to systolic-diastolic mobility restriction (Fig.1). This resulted in massive TR (VC 16 mm, ERO 1.6 cm², dense triangular CW Doppler profile and systolic flow reversal in suprahepatic veins, Fig.2) combined with tricuspid stenosis (mean gradient 5 mmHg). Crucially, detailed evaluation of the pulmonary valve revealed retracted cusps. Diagnosis of pulmonary regurgitation (PR) was challenging at Color Doppler but a multiparametric assessment detected severe PR (dense CW Doppler with rapid interruption due to a rapid rise of RV diastolic pressures with pressure half-time of 80 msec and PR index of 0,62, Fig.3). Conclusion: These findings are pathognomonic for CHD, where vasoactive substances (e.g., serotonin) induce endocardial fibrosis. In this case, the complex anatomy of the tricuspid valve, combined with significant pulmonary valve involvement, rendered the patient unsuitable for transcatheter correction. This case emphasizes that the pulmonary valve must be rigorously evaluated in CHD, with a multiparametric approach, as its involvement is a critical determinant of surgical vs. percutaneous strategy. Management in this case must involve a multidisciplinary Heart Team to balance surgical risks against oncological prognosis.