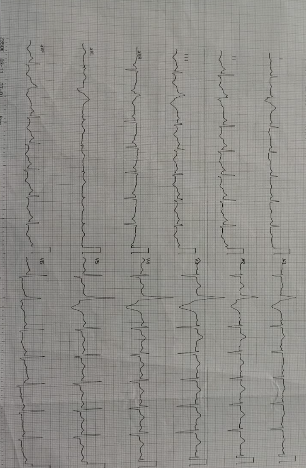
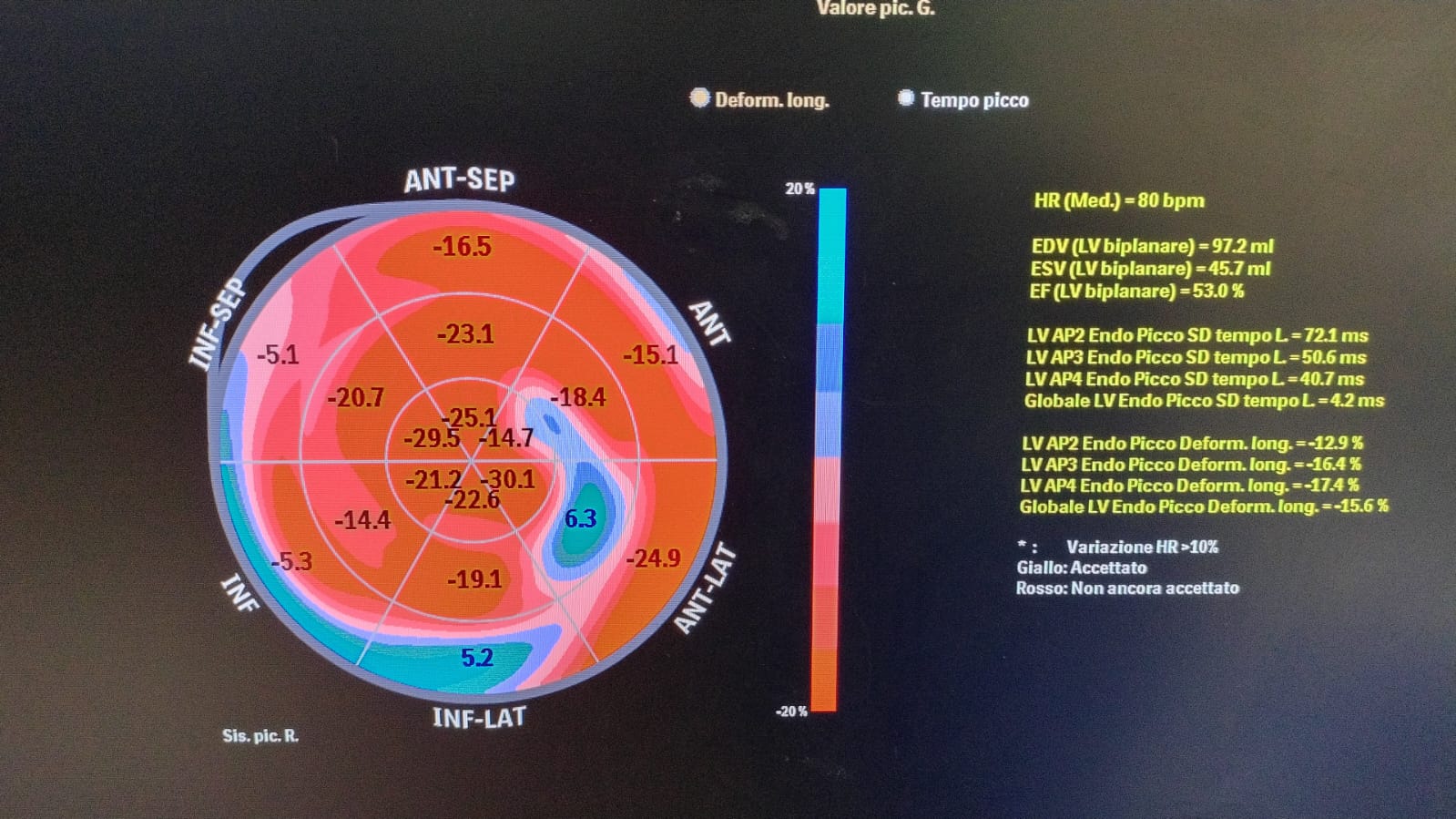
A 42-year-old woman experienced an out-of-hospital cardiac arrest (OHCA) at her home, presenting with ventricular fibrillation (VF). She was successfully resuscitated with three DC shocks and transported to our hospital in return of spontaneous circulation (ROSC). The patient had no notable medical history, cardiovascular risk factors, or family history, and was only taking oral contraceptives at home. Upon arrival in the emergency department (ED), she was agitated and non-responsive. Her blood pressure was 115/70 mmHg, and she was eupneic without oxygen support. ECG showed negative T waves in leads AVF and DIII. Occasional premature ventricular beats (PVB) were noted originating from the inferior wall of the left ventricle. Echocardiography revealed good biventricular function, mitral valve prolapse, and evidence of pseduo-mitral annular disjunction (pseudoMAD) with 7mm of disjunction in systole, which led to severe mitral regurgitation (MR). Pichelhaube’s sign was noted No reversible causes were identified. Due to her extreme agitation and recent arrhythmic storm, she was intubated, mechanically ventilated, and transferred to the intensive care unit (ICU). Antiarrhythmic therapy with propranolol 80 mg/day and amiodarone was initiated. The following day, the patient was successfully extubated without neurological deficits and transferred to our coronary intensive care unit (UTIC). Follow-up echocardiography showed improvement in mitral regurgitation (now moderate), and a focal reduction in global longitudinal strain (GLS) was observed in the basal posterolateral and inferior walls. A contrast-enhanced chest CT ruled out pulmonary embolism, and coronary angiography revealed no significant lesions. A transesophageal echocardiogram confirmed psuedoMAD and moderate mitral insufficiency. Subsequently, she underwent implantation of a subcutaneous implantable cardioverter defibrillator (S-ICD). The patient was discharged asymptomatic on medical therapy with propranolol 60 mg/day. During her stay in UTIC, no further arrhythmic events occurred. Cardiac MRI revealed a transmural late gadolinium enhancement (LGE) area in the basal inferior, posterolateral, and septal walls, also pseudoMAD was confirmed. This case highlights the complexity of diagnosing and managing pseudoMAD, especially in the context of life-threatening arrhythmias.