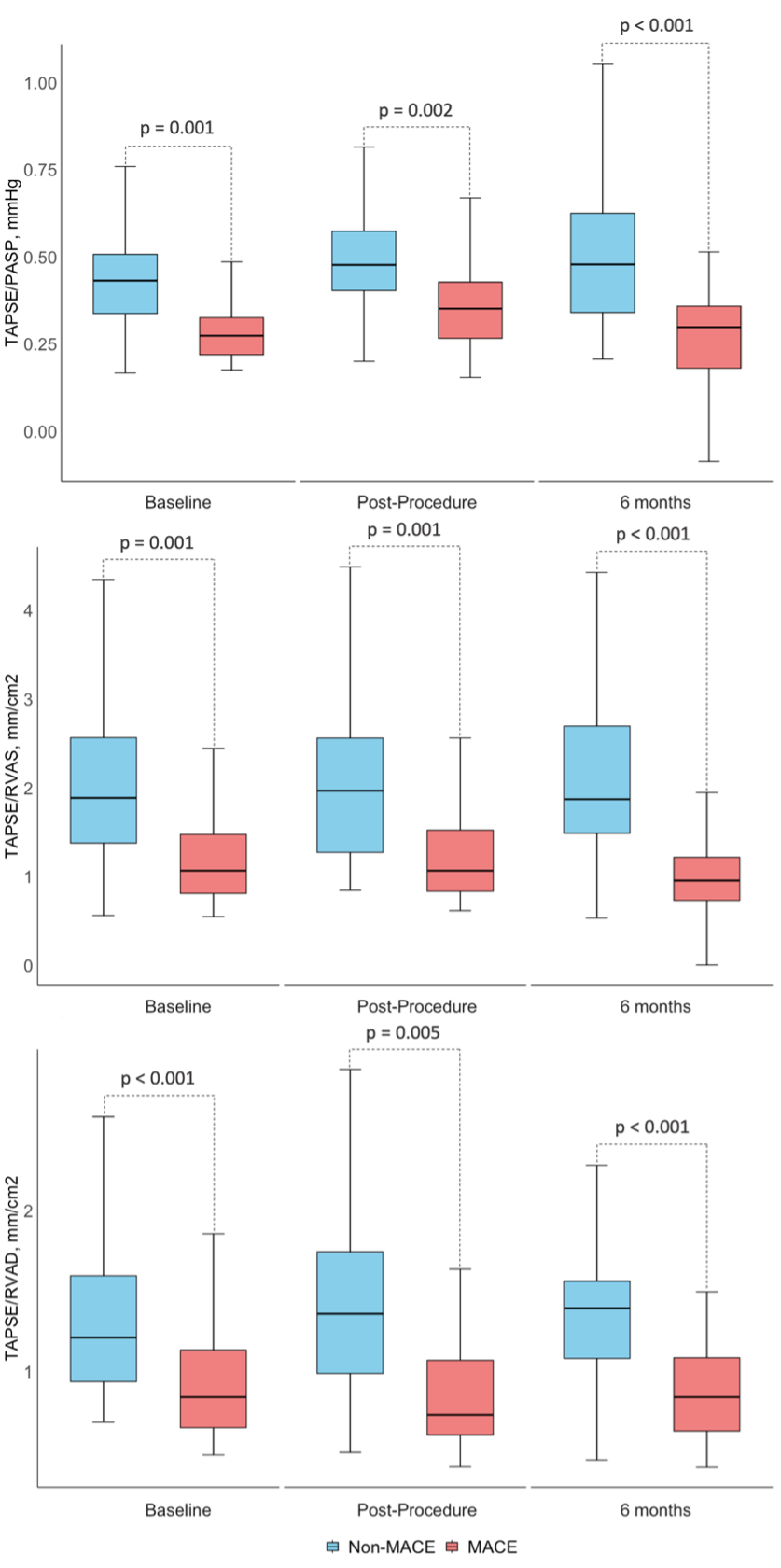
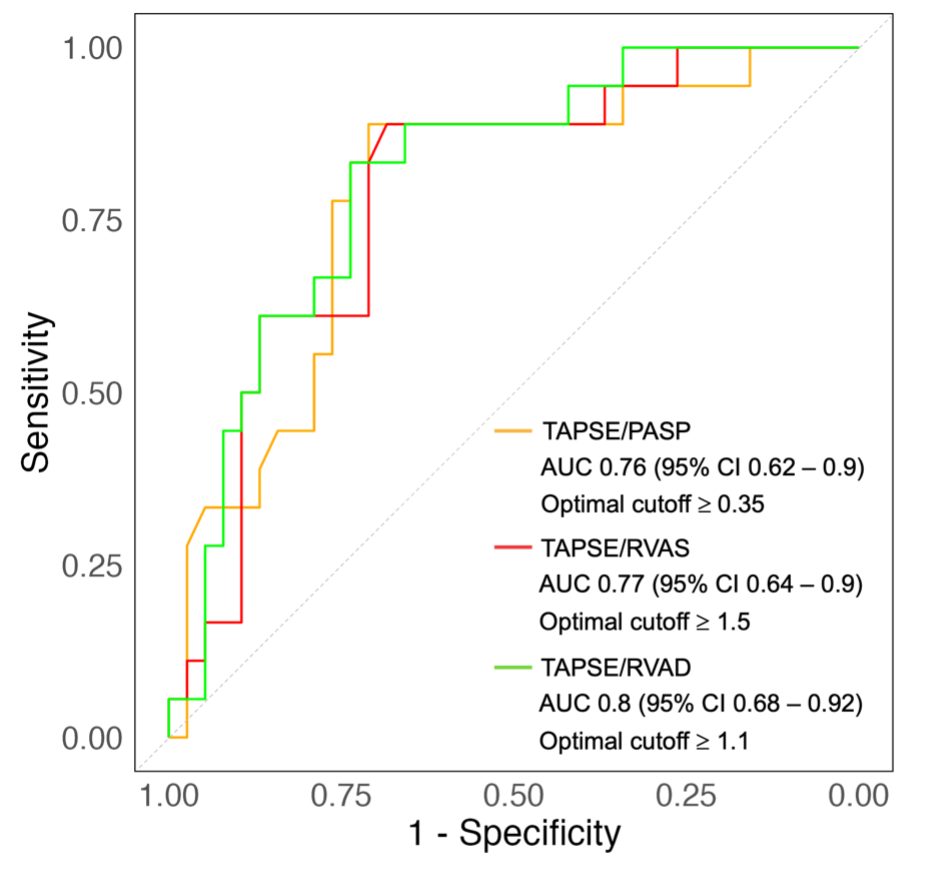
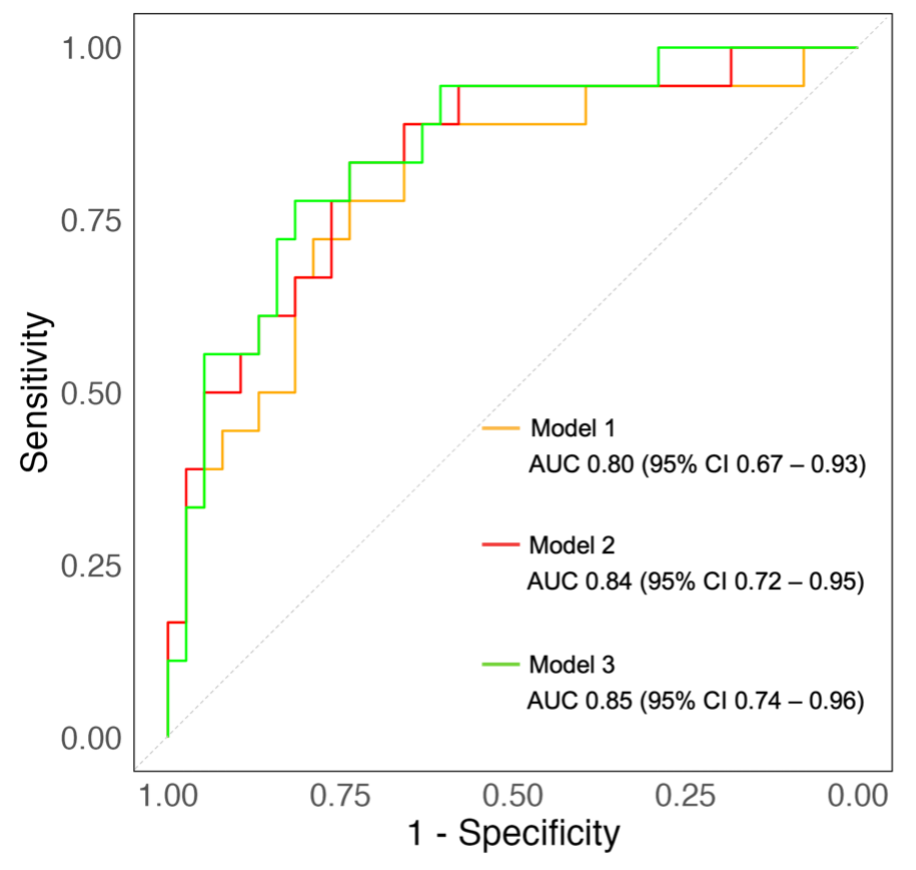
Background Mitral regurgitation (MR) is a prevalent valvular heart disease with poor outcome. Percutaneous mitral valve repair on top of guidelines-directed medical therapy has been associated with prognostic benefit. Yet, the percentage of patients who die or are re-hospitalized for heart failure, within the first year is high. Identification of these short-term non-responders to PMVR is of great clinical importance. Aims This study aims to assess the prognostic value of advanced right ventricular (RV) function parameters in predicting major adverse cardiovascular events (MACE) following percutaneous mitral valve repair using the MitraClip system. Methods This study analysed 60 consecutive patients with symptomatic severe MR who underwent percutaneous mitral valve repair . Echocardiographic assessments were performed at baseline, post-procedure before discharge, and at 6-month follow-up. Analysed echocardiographic parameters included tricuspid annular plane systolic excursion (TAPSE) normalized either to pulmonary artery systolic pressure (TAPSE/PASP), or to RV end-diastolic (TAPSE/RVAD) and end-systolic area (TAPSE/RVAS), and indices of RV myocardial work. MACE including all-cause death, heart failure hospitalization, and stroke, was assessed at one year of follow-up. Results A total of 35% of patients experienced MACE during the first year after percutaneous mitral valve repair . At baseline, patients with versus without MACE had significantly higher creatinine, troponin T, NT-proBNP and larger right heart size and lower TAPSE (all p < 0.05) while the remaining clinical, imaging and procedural characteristics were similar. In multivariate regression analysis, TAPSE/PASP, TAPSE/RVAS and TAPSE/RVAD were only significant imaging predictors of MACE (all p < 0.05). The AUC values using the multivariate models ranged from 0.80 to 0.85, indicating moderate to strong predictive capacity for these RV indices. Throughout the follow-up, these indices of RV function remained significantly lower in patients with versus without MACE (all p < 0.05). In contrast, parameters of RV myocardial work had significantly lower AUC (< 0.60) across all the time points. Conclusion The results of the present study suggest that the comprehensive assessment of the right ventricle can identify short-term non-responders to PMVR. The indices including TAPSE emerged as independent predictors of outcome while the indices based on RV myocardial work showed limited predictive power.