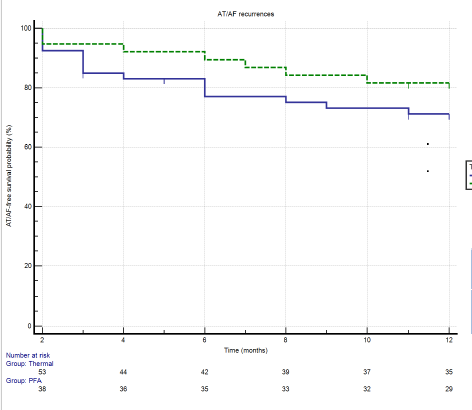
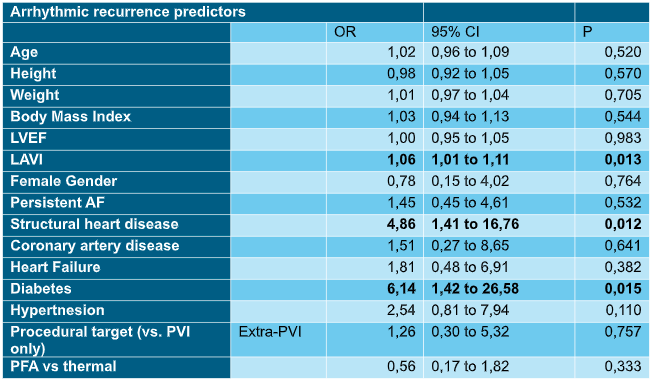
Pulsed Field Ablation (PFA) is a mainly non-thermal energy source capable of creating myocardial-selective lesions. This study evaluated efficacy and safety of its introduction into real-world clinical practice for atrial fibrillation (AF) ablation. A retrospective analysis was conducted on all consecutive patients treated with AF ablation between January 2022 and September 2024 at our center, evaluated according to the energy source used (i.e. PFA vs thermal ablation). The primary efficacy endpoint was one-year recurrence of any sustained atrial tachyarrhythmia; major procedural complications represented the safety endpoint. Predictors of recurrence were studied using logistic regression analysis. A total of 117 patients (70 thermal and 47 PFA; 96 first procedure and 21 redo) were included in our analysis. Mean age was 61±9 years, and 82% were male. Persistent AF was present in 44 patients (38%) and 25 had structural heart disease (21%). Median left ventricle ejection fraction (LVEF) was 60% (IQR 54-65%), and medial left atrial volume index (LAVI) was 40 ml/m 2 (IQR 33-50). Twelve-month follow-up was completed in 91 patients (53 thermal and 38 PFA), while the follow-up analysis of first procedures included 74 patients (43 thermal and 31 PFA). One-year recurrence rates were not significantly different between groups (28.3% in the thermal cohort vs 18.4% in the PFA cohort, p=0.242). When only first procedures were considered, recurrence remained comparable (25.6% vs 16.1% p= 0,303 – Figure 1). Safety outcomes were similarly consistent, with no significant difference in major complications between groups (5.7% vs 4.3% in thermal and PFA group, respectively p=1,000), mainly driven by vascular access complications (3.4% vs 5.4%, p=0,414). Logistic regression identified LAVI (OR 1.06, 95% CI 1.01–1.11, p=0.013), structural heart disease (OR 4.86, 95% CI 1.4–16.8, p=0.012), and a history of diabetes mellitus (OR 6.14, 95% CI 1.4–26.6, p=0.015) as predictors of arrhythmic recurrence after a first ablation procedure (Table 1). This single-center real-world experience confirms the favorable efficacy and safety profile of PFA for AF ablation, which was overall comparable to that of traditional thermal modalities.Left atrial enlargement, structural heart disease and diabetes emerged as the strongest predictors of AF recurrence at one-year follow-up.