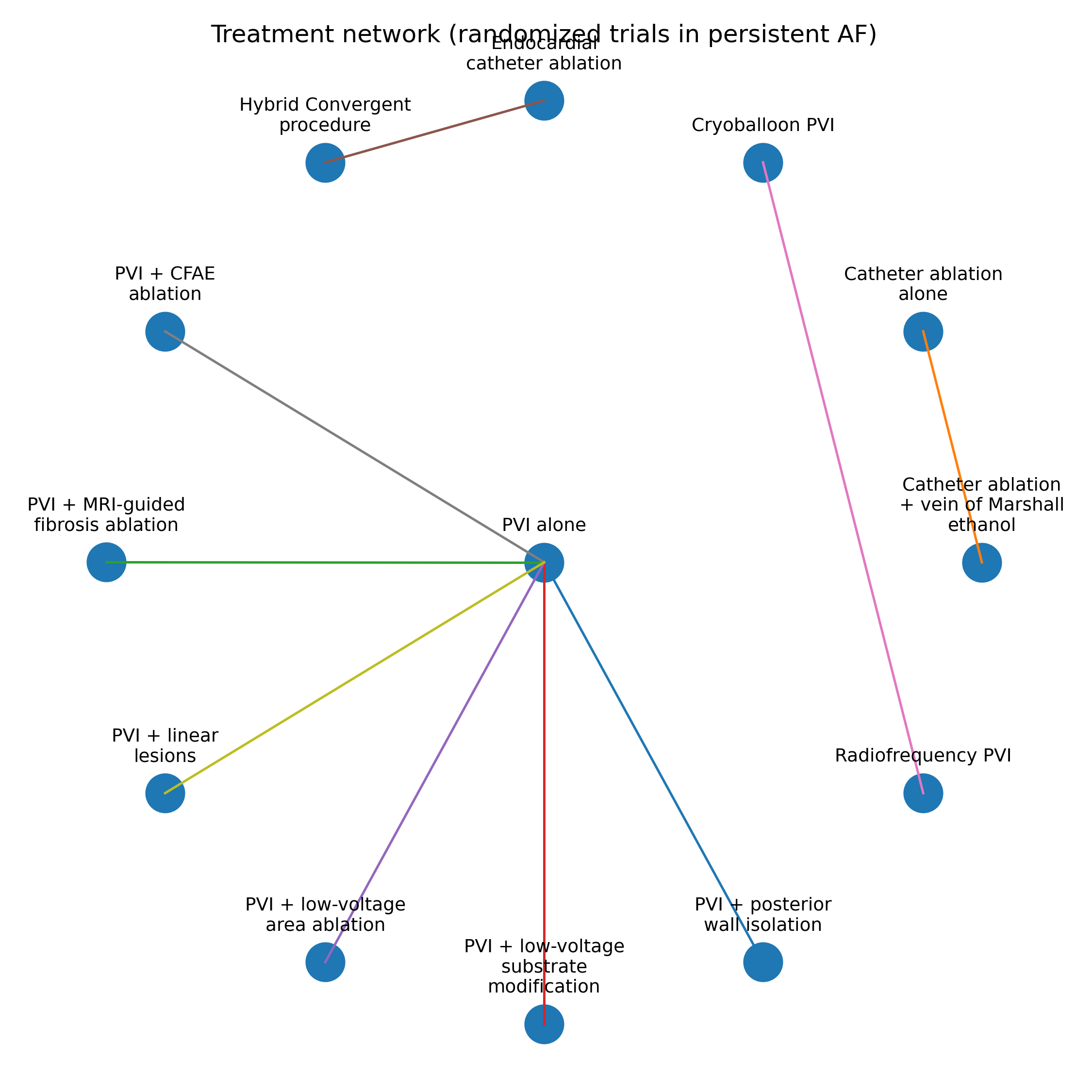
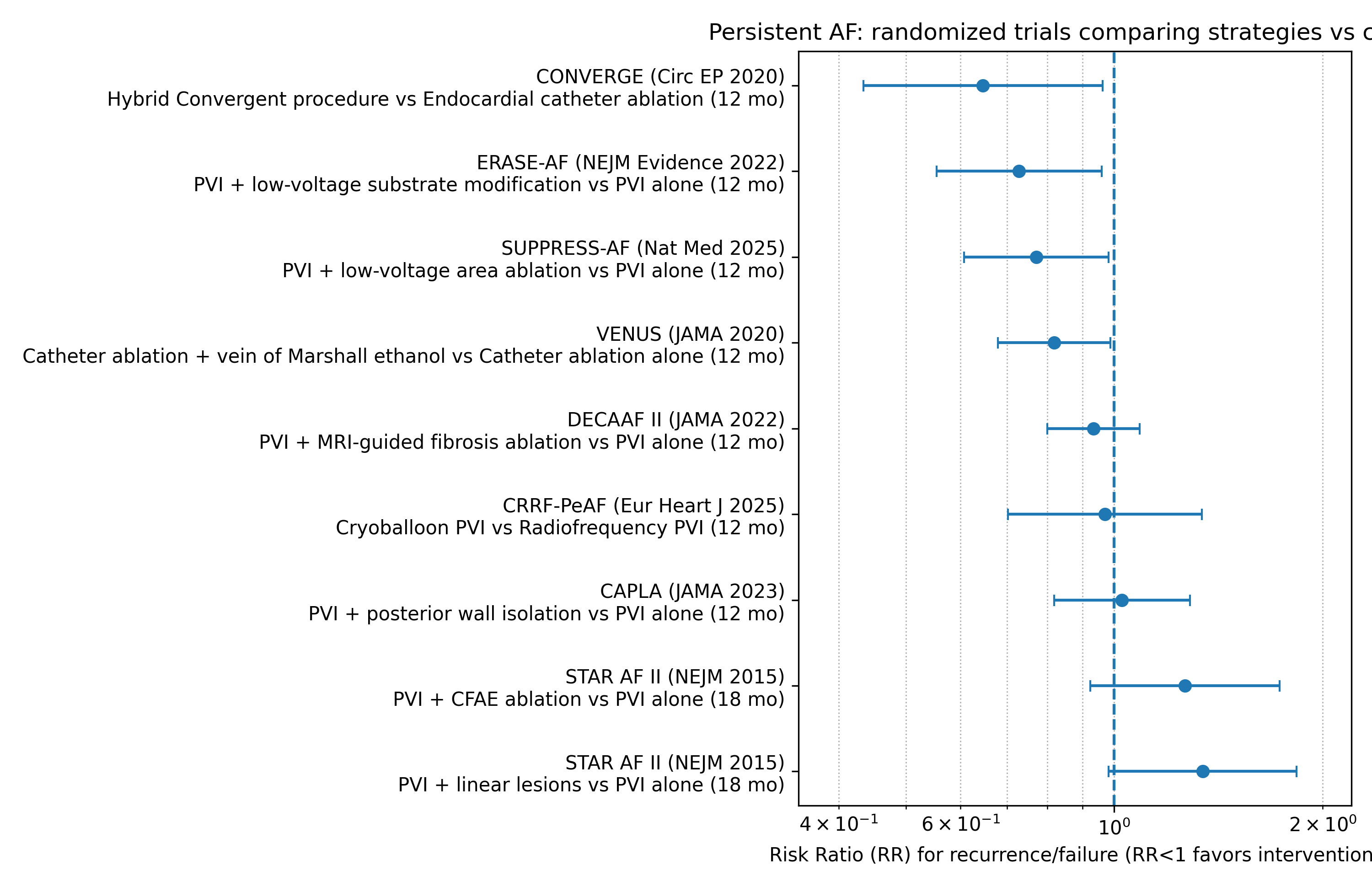
Background: Pulmonary vein isolation (PVI) remains the cornerstone of catheter ablation in persistent atrial fibrillation (PersAF), yet recurrence is frequent. Multiple adjunctive strategies have been tested with heterogeneous results. Methods: We performed a focused synthesis of major randomized controlled trials (RCTs) in PersAF comparing PVI-based catheter ablation with adjunctive or alternative strategies. The primary endpoint was atrial tachyarrhythmia recurrence/failure at ~12 months after a 90-day blanking period. Effects are presented as risk ratios (RR) for recurrence/failure (RR<1 favors intervention). A sensitivity analysis included STAR AF II (18-month follow-up). Results: Nine randomized comparisons were included (CAPLA, VENUS, DECAAF II, ERASE-AF, SUPPRESS-AF, CONVERGE, CRRF-PeAF, and two STAR AF II arms), encompassing >3,000 patients overall. Routine posterior wall isolation did not reduce recurrence vs PVI (52.4% vs 53.6% free; HR≈0.99). MRI-guided fibrosis ablation also showed no benefit and increased safety events (43.0% vs 46.1% recurrence; HR≈0.95). In contrast, strategies targeting non-PV substrate showed favorable signals: vein of Marshall ethanol improved freedom from arrhythmia (49% vs 38%). Low-voltage substrate modification reduced recurrence (35% vs 50%). LVA-guided ablation improved 1-year arrhythmia-free survival (61% vs 50%; HR≈0.78). Hybrid Convergent outperformed endocardial catheter ablation (67.7% vs 50.0% effectiveness). Cryoballoon was non-inferior to radiofrequency. CFAE/linear lesions did not improve outcomes. Conclusions: In PersAF, empiric anatomic lesion sets (posterior wall, CFAE/lines) and MRI-guided fibrosis ablation do not meaningfully reduce recurrence, whereas mechanistic substrate approaches (VOM ethanol, low-voltage targeting) and hybrid epicardial-endocardial ablation show the most consistent signals toward lower recurrence, warranting further head-to-head trials.