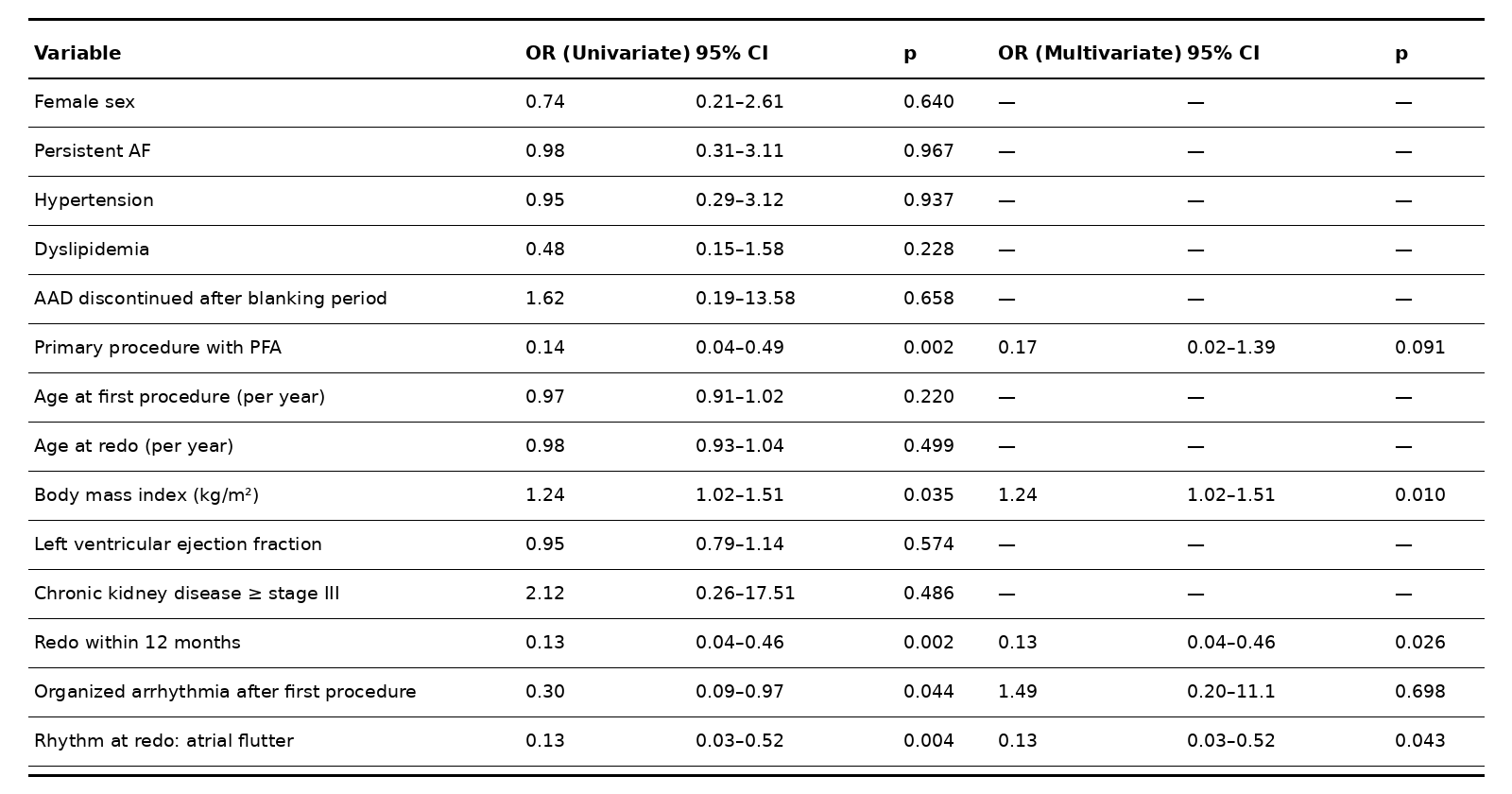
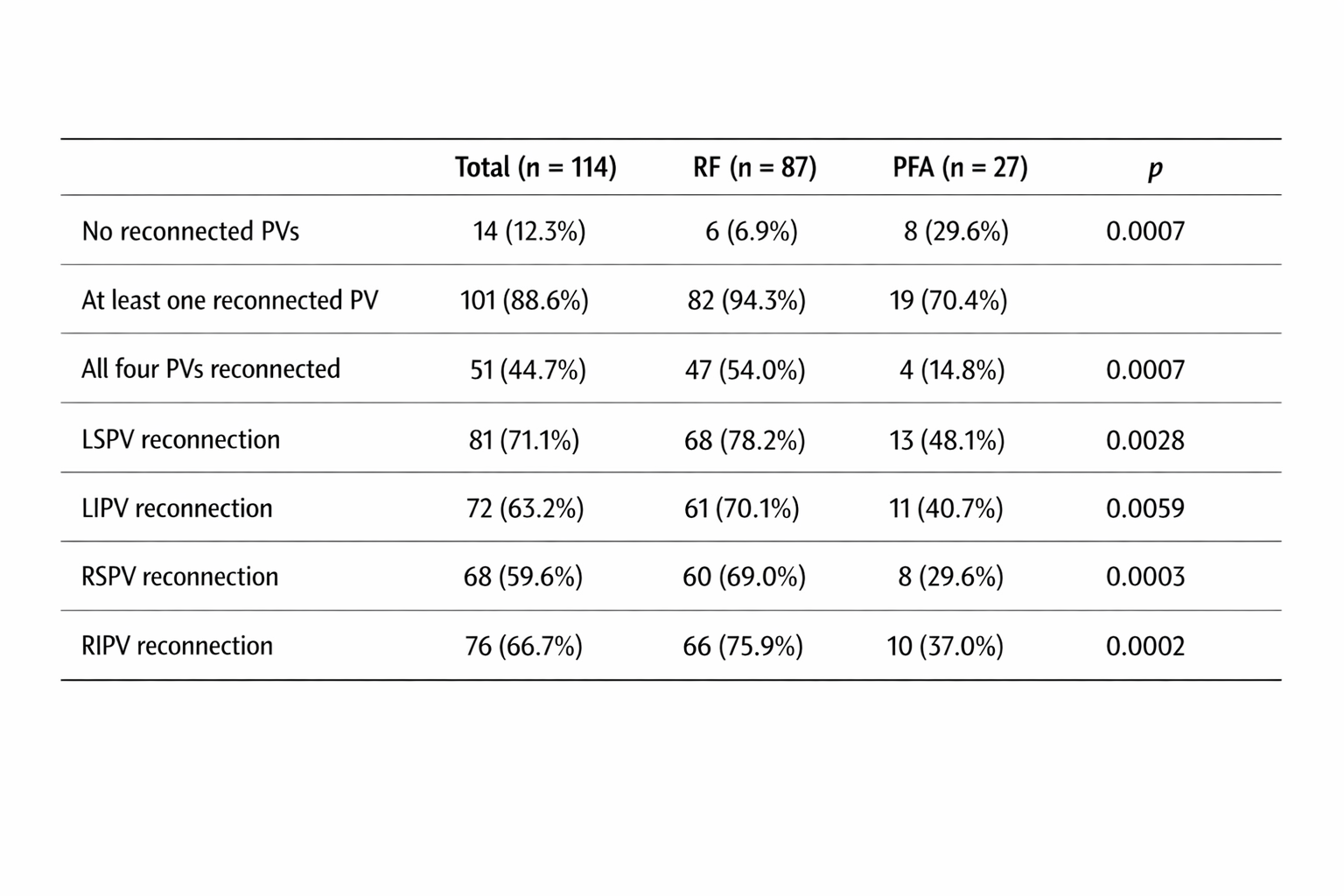
Introduction Pulmonary vein (PV) isolation durability is a major determinant of long-term success after atrial fibrillation (AF) ablation. Pulsed field ablation (PFA) has emerged as an alternative to radiofrequency (RF), potentially offering more homogeneous and durable lesions. However, real-world data comparing PV reconnection rates between these technologies at repeat procedures are still limited. Methods We performed a multicenter retrospective analysis of patients undergoing a repeat ablation procedure for arrhythmic recurrence after a first AF ablation performed with RF or PFA. High-density electroanatomical mapping was systematically used to assess PV reconnection. The primary endpoint was the presence of at least one reconnected PV. Secondary analyses included the number and distribution of reconnected PVs and the identification of predictors of PV reconnection. Results A total of 114 patients were included; 87 (76%) had undergone RF ablation and 27 (24%) PFA at the index procedure. Overall, 101 patients (89%) showed at least one reconnected PV at redo. PV reconnection was significantly more frequent in the RF group compared with PFA (94% vs 70%, p < 0.001), and reconnection of all four PVs occurred predominantly after RF ablation (54% vs 15%, p < 0.001). For each individual PV, reconnection rates were consistently lower in the PFA group (Table 1). Use of PFA at the index procedure was associated with a significantly lower rate of PV reconnection at univariate analysis (OR 0,15; 95% CI 0.04–0.50; p = 0.002). Nonetheless, energy source lost significance in multivariate analysis (p=0,09 – Table 2). On the other hand, redo ablation performed within 12 months from the index procedure (OR 0.1, 95% CI 0.01–0.76; p = 0.026) and presentation with atrial flutter at admission for redo (OR 0.09, 95% CI 0.01–0.92; p = 0.043) were independently associated with a lower risk of PV reconnection, and a higher body mass index (BMI) emerged as an independent predictor of PV reconnection (OR 1.52, 95% CI 1.1–2.1; p = 0.010). Conclusion In this multicenter real-world cohort of redo AF ablation procedures, PFA showed high rates of durable PV isolation over time. However, the multivariate analysis suggests that the time to redo procedure significantly impacts reconnection rates; therefore, further studies with longer follow-up are required to evaluate its definitive superiority over RF and clarify the mechanisms underlying lesion durability with different energy sources.