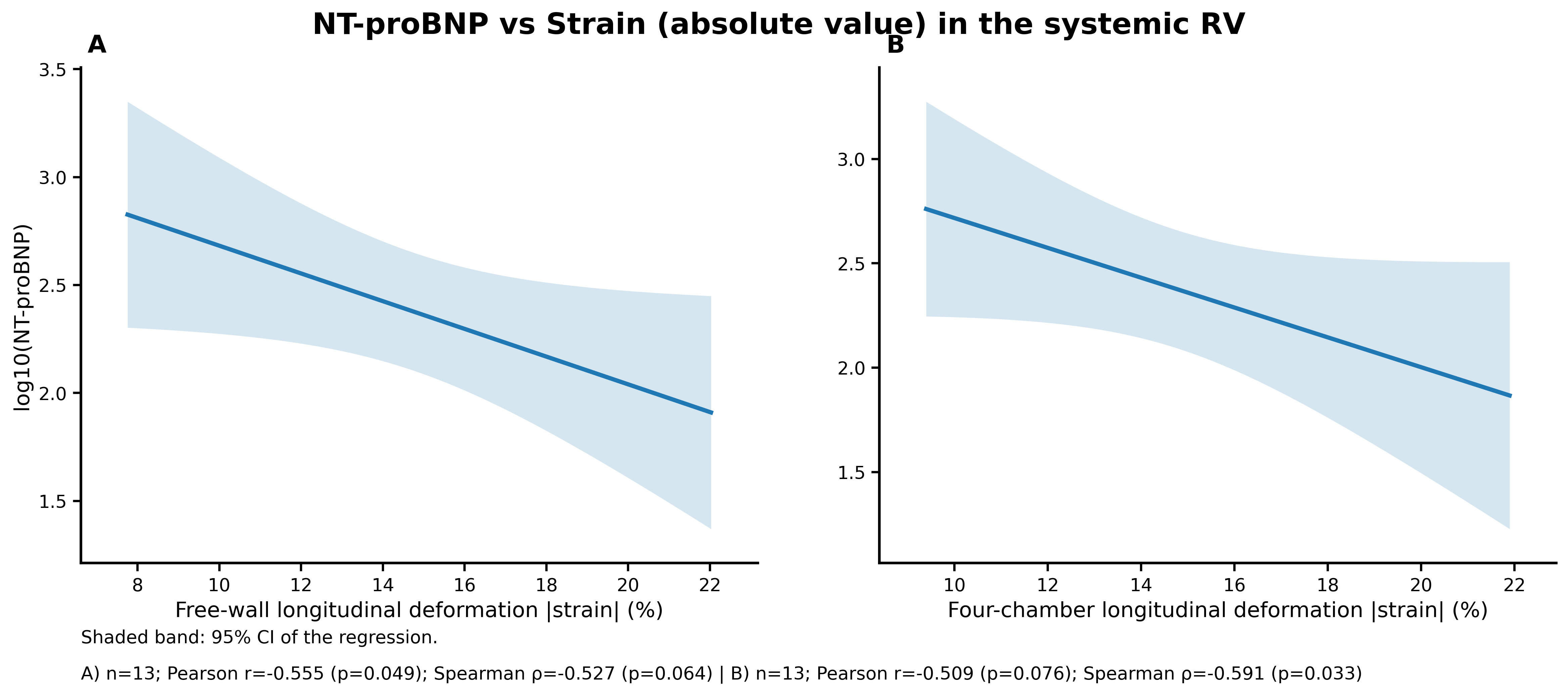
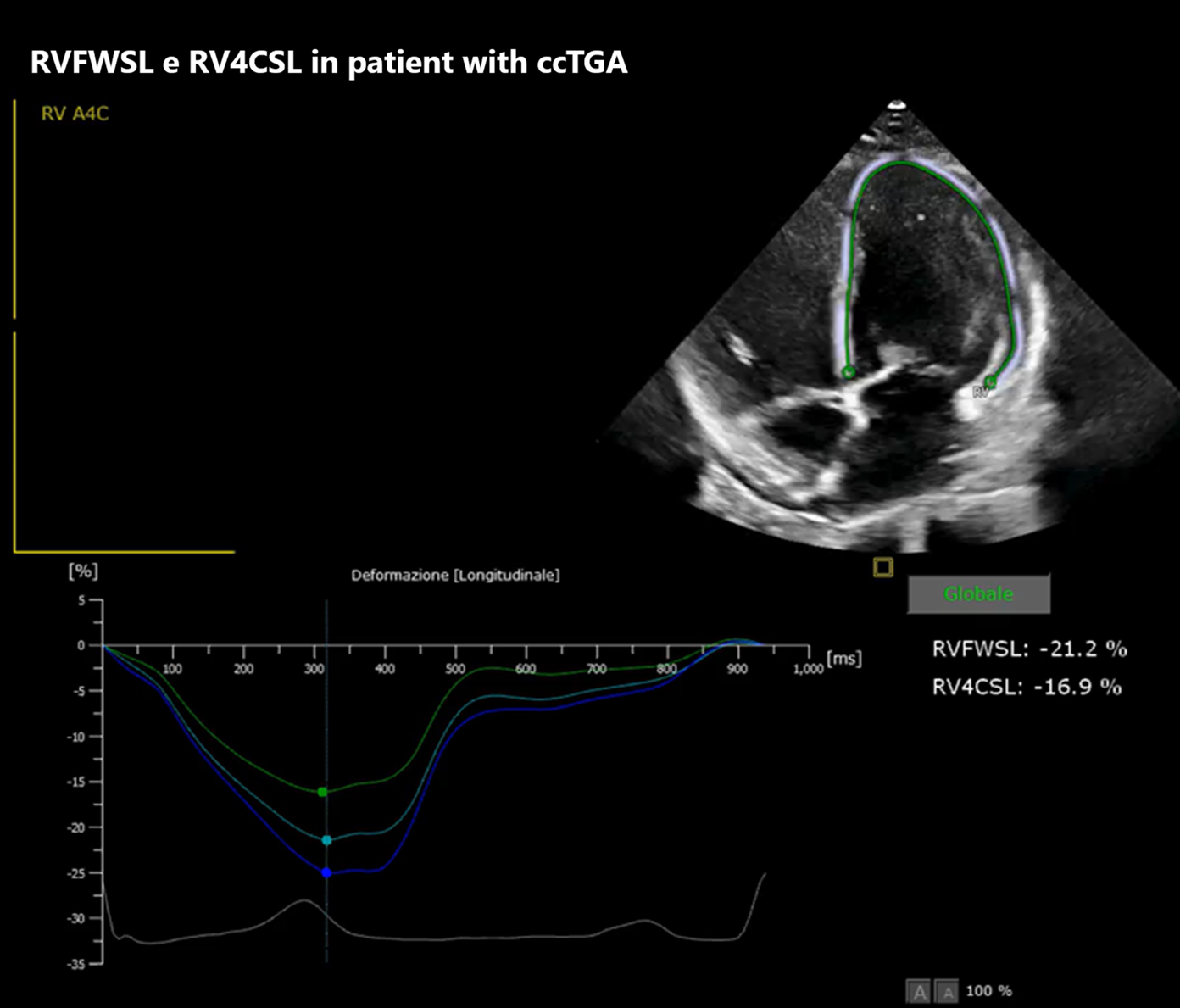
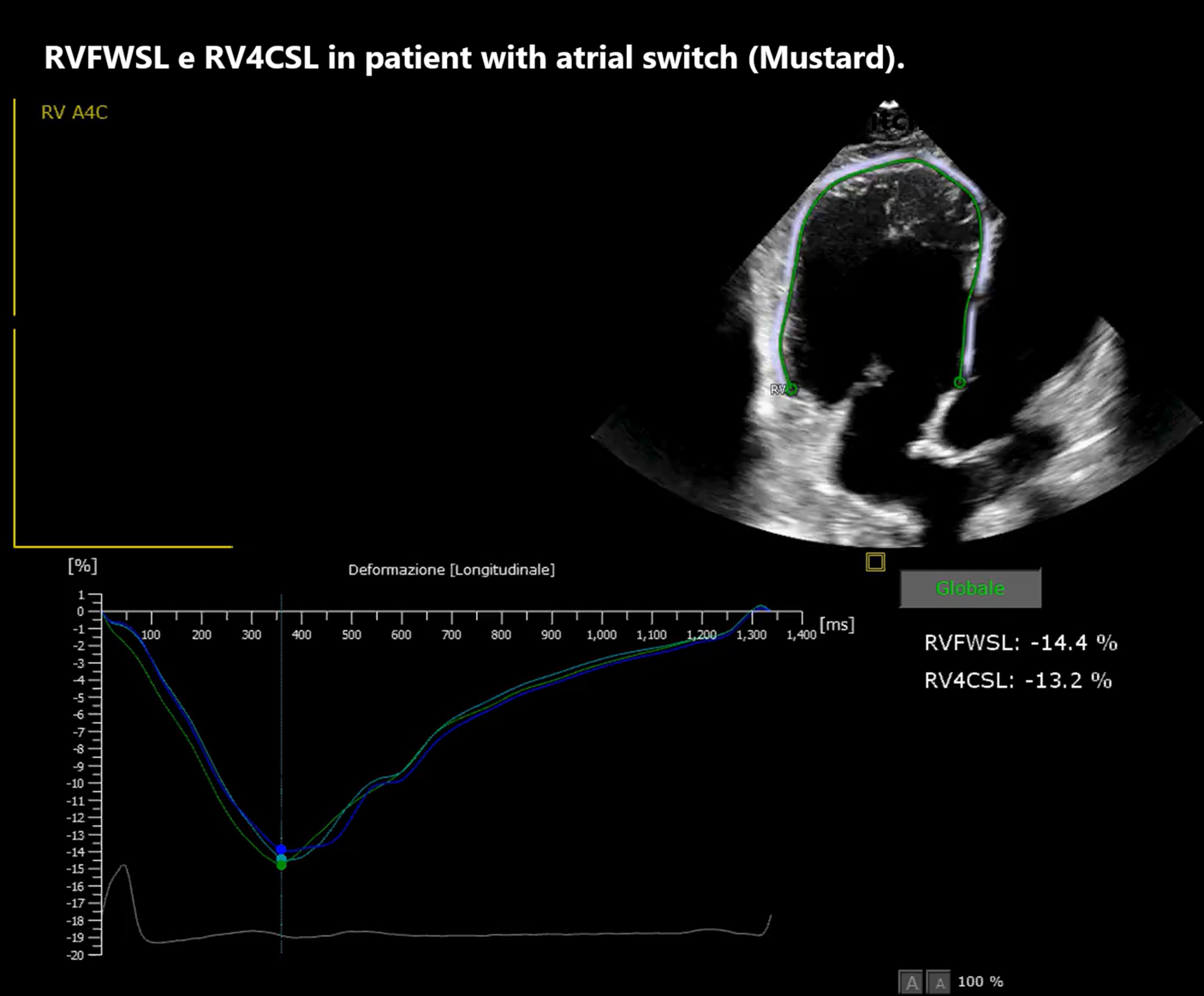
Background: The systemic right ventricle (sRV), present in patients with d-TGA after atrial switch and in congenitally corrected TGA (ccTGA), is chronically pressure-loaded, leading to ventricular remodeling and progressive dysfunction. In this setting, markers of myocardial mechanics and wall stress integrating imaging and biomarkers are useful. Aim: To evaluate the association between NT-proBNP and sRV longitudinal strain (four-chamber strain, RV4CSL, and free-wall strain, RVFWSL) and, secondarily, to describe its relationship with conventional echocardiographic indices (FAC, TAPSE, TDI S′) in a GUCH cohort with sRV in biventricular circulation (Mustard/Senning and ccTGA). Methods: Retrospective study of 20 patients followed at our Center (ARNAS Civico–Di Cristina, Pediatric Cardiology Unit). All underwent comprehensive clinical assessment with functional evaluation, laboratory testing, ECG/Holter and echocardiography; speckle-tracking strain was available in 13/20 patients. Associations were explored using linear models and Pearson correlation; NT-proBNP was also log-transformed (log10) and results were checked with Spearman as a sensitivity analysis for outliers. Results: In patients with complete echocardiographic strain and NT-proBNP data (n=13), RVFWSL was inversely associated with NT-proBNP (Pearson r=−0.555; p=0.049; Spearman ρ=−0.527; p=0.064), suggesting that reduced longitudinal deformation (less negative strain values) is accompanied by greater neurohormonal activation. RV4CSL also showed a consistent inverse association with NT-proBNP (Pearson r=−0.509; p=0.076; Spearman ρ=−0.591; p=0.033), with less negative RV4CSL values associated with higher NT-proBNP. As a complementary analysis, higher FAC was associated with higher absolute RV4CSL (r=0.624; p=0.023), whereas TAPSE and TDI S′ showed weaker but concordant associations. Conclusions: In our biventricular-circulation sRV cohort, higher NT-proBNP is associated with worse longitudinal mechanics, particularly at the free wall. Interpreted together, strain and NT-proBNP may help grade hemodynamic severity and guide follow-up; these exploratory findings require confirmation, using additional diagnostic modalities.