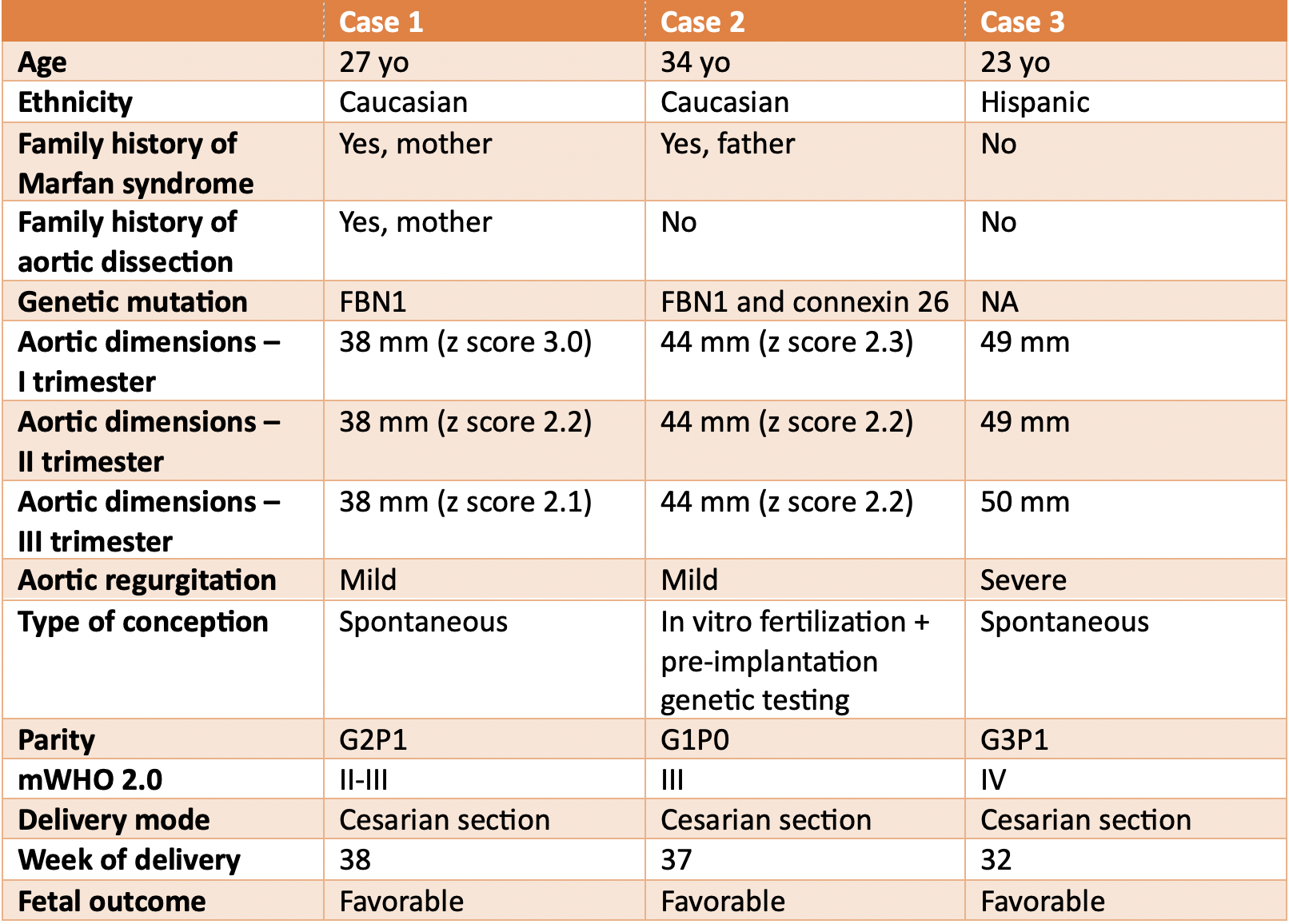
Background: Pregnancy in women with Marfan syndrome (MFS) carries a high risk of cardiovascular complications, particularly aortic dissection, due to hemodynamic and hormonal changes. Multidisciplinary management of pregnancy and delivery and continue risk reassessment are essential to minimize maternal and fetal complications. Case Series: We report three cases of women with MFS managed at our cardio-obstetric clinic during pregnancy (table 1). A 27-year-old woman with familial MFS (pathogenic FBN1 mutation) was referred at 12 weeks during her second pregnancy. She was in mWHO class II-III and started on low-dose beta-blocker for heart rate and blood pressure control. Echocardiography showed stable aortic root dimensions throughout pregnancy, and regular fetal growth. Due to previous cesarean section, the patient was assigned to cesarean delivery, successfully performed at 38w with general anaesthesia due to dural ectasia which contraindicated spinal anaesthesia. A 34-yo woman with familial MFS (carrier of double mutation of FBN1 and connexin 26) had a planned pregnancy with in-vitro fertilisation and pre-implant genetic testing. Angiotensin-II receptor-blocker was discontinued upon pregnancy confirmation, and the patient was kept on beta-blocker. Echocardiography revealed a stable aortic root dilatation associated with mitral annular disjunction. Cesarean section was performed at 37w due to mWHO Class III. The third case, a 23-yo woman, was referred at 12w due to suspected MFS (aortic root 49 mm, severe aortic regurgitation). She was started on beta-blocker and continued pregnancy under close follow-up. Due to mWHO Class IV and worsening chest pain, caesarean section was performed at 32w with cardiac surgery back-up, without maternal or fetal complications. Conclusion: Pregnancy in MFS requires individualized, multidisciplinary care. Early risk assessment, with re-evaluation throughout the whole pregnancy, close monitoring with serial echocardiograms, and coordination among cardiologists, obstetricians, anaesthesiologists, and cardiac surgeons are crucial to optimize both maternal and fetal outcomes.