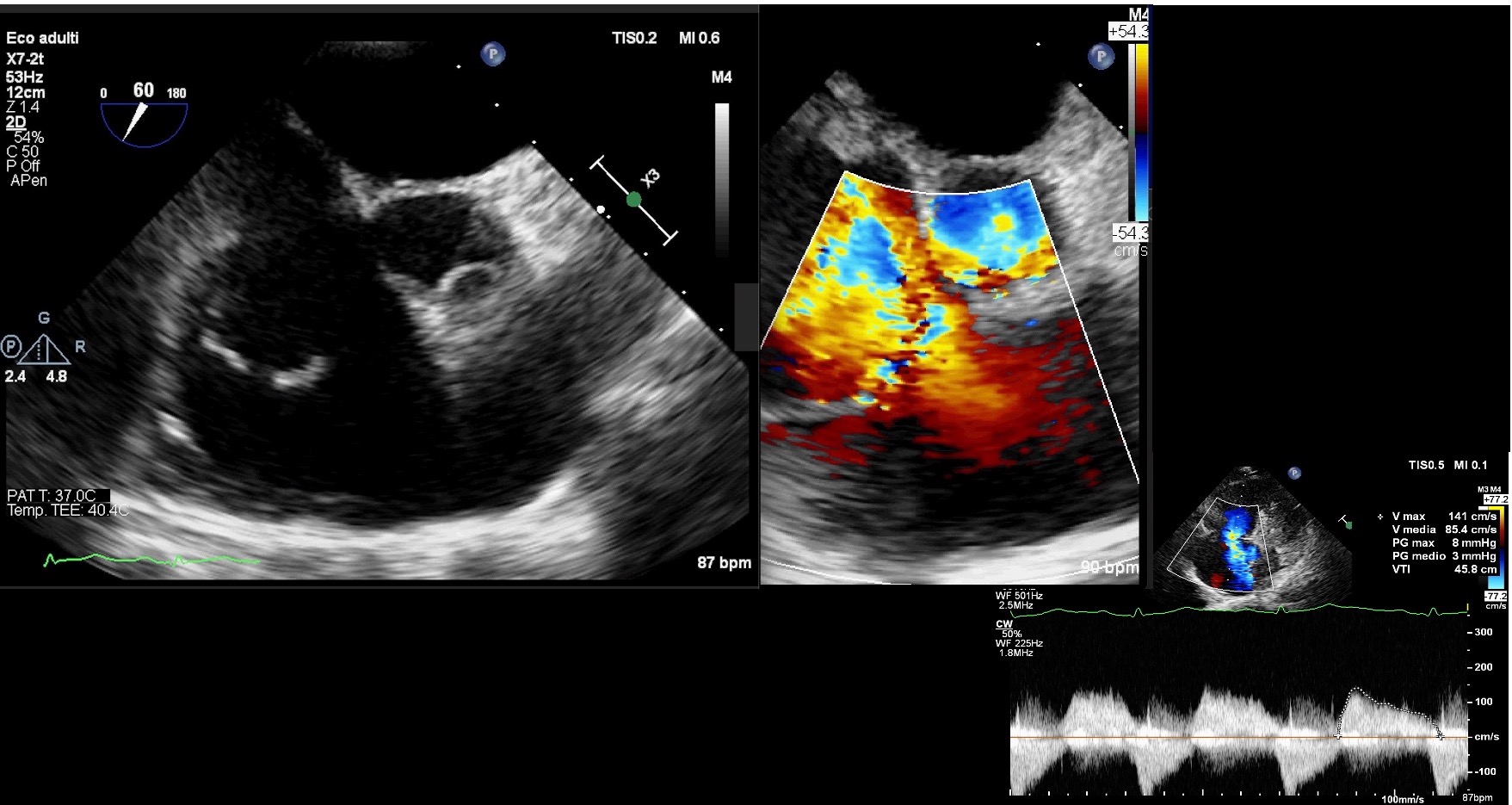
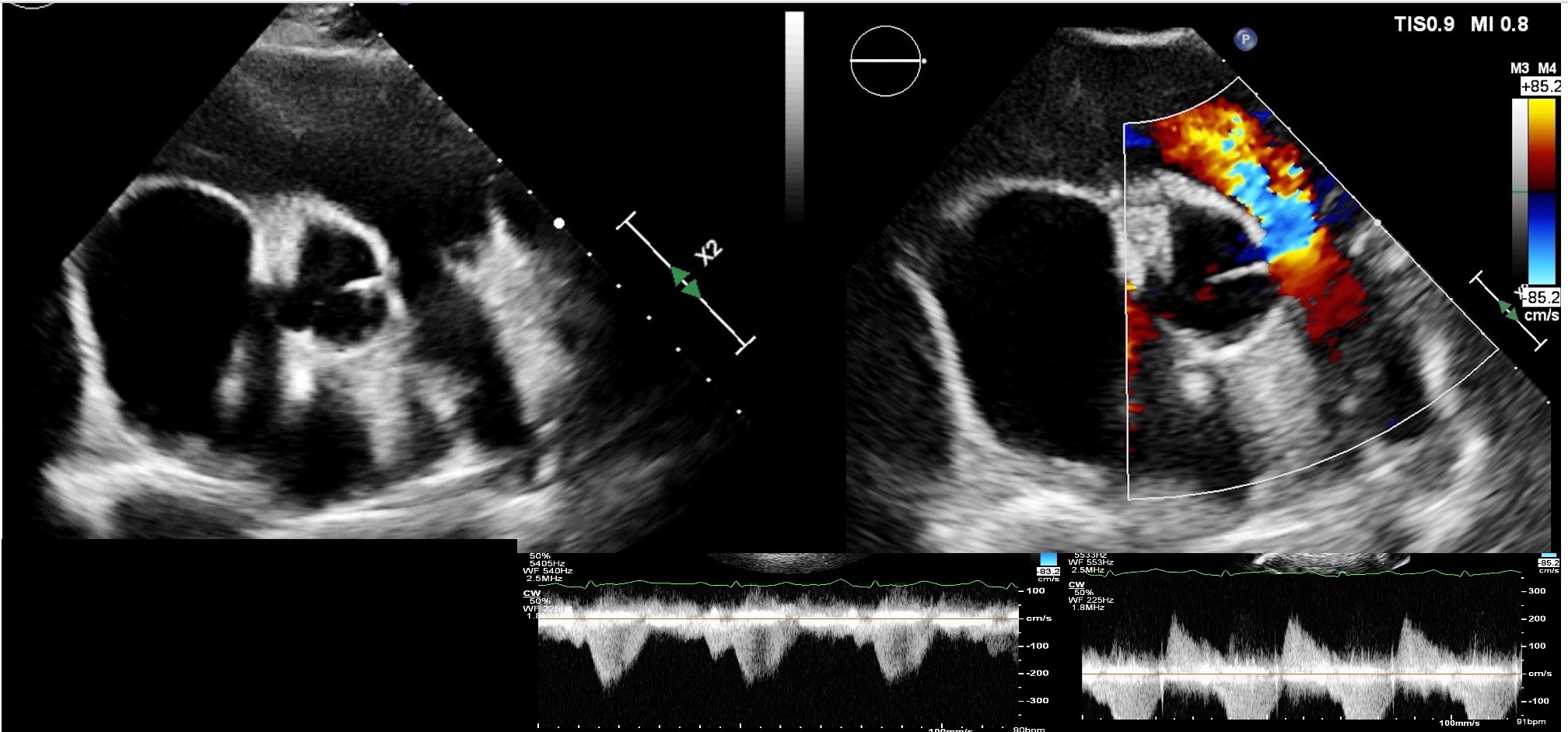
A 65 year-old hypertensive woman came to our attention for exertional dyspnoea (NYHA II), peripheral oedema and weight gain. The general practitioner started a low dose of loop diuretic with partial benefit. At physical examination she presented a 2/6 systolic murmur and all signs of right heart failure. A quick-look echocardiographic evaluation showed significant dilation of right chambers with preserved systolic function of the right ventricle, significant tricuspid regurgitation and signs of visceral congestion. Pulmonary embolism was excluded by CT pulmonary angiogram. The patient was admitted to the cardiac unit, and treated with loop diuretic, mineralocorticoid receptor antagonist, beta-blocker and ACE-inhibitor. Transthoracic echocardiogram showed a significant dilation of right atrial and ventricular chambers, with diastolic flattening of the interventricular septum, suggesting right ventricular volume overload. The systolic function of the right ventricle was preserved. At transesophageal echocardiographic evaluation, tricuspid valve was severely affected (Fig.1), with leaflets appearing thickened, retracted and fixed in a semi-open position, causing severe tricuspid regurgitation without significant stenosis (mean gradient of 3 mmHg). Pulmonary valve was also involved (Fig.2), with leaflets appearing severely retracted and shortened, together with narrowing of the valvular annulus (annular diameter 1.3 cm), causing severe pulmonary regurgitation with color flow doppler occupying the entire pulmonary outflow tract, and mild stenosis (mean/maximum gradient of 12/23 mmHg). Left side structures were not affected. Right heart cardiac catheterization confirmed both the right ventricle dilation and the massive tricuspid regurgitation. It also showed significant right atrial enlargement with right atrial pressure wave form comparable to the observed in the ventricle. The peculiar characteristics of both tricuspid and pulmonary valve led to the suspicion of a carcinoid syndrome, considering that a congenital heart disease was unlikely due to the advanced age of the woman. The patient underwent an abdominal CT scan that showed several metastatic liver lesions. High level of serum chromogranin A and urinary 5-hydroxindolacetic acid were consistent with a neuroendocrine tumor. The intestinal biopsy of ileocecal valve and of liver lesions confirmed the diagnosis of neuroendocrine tumor.