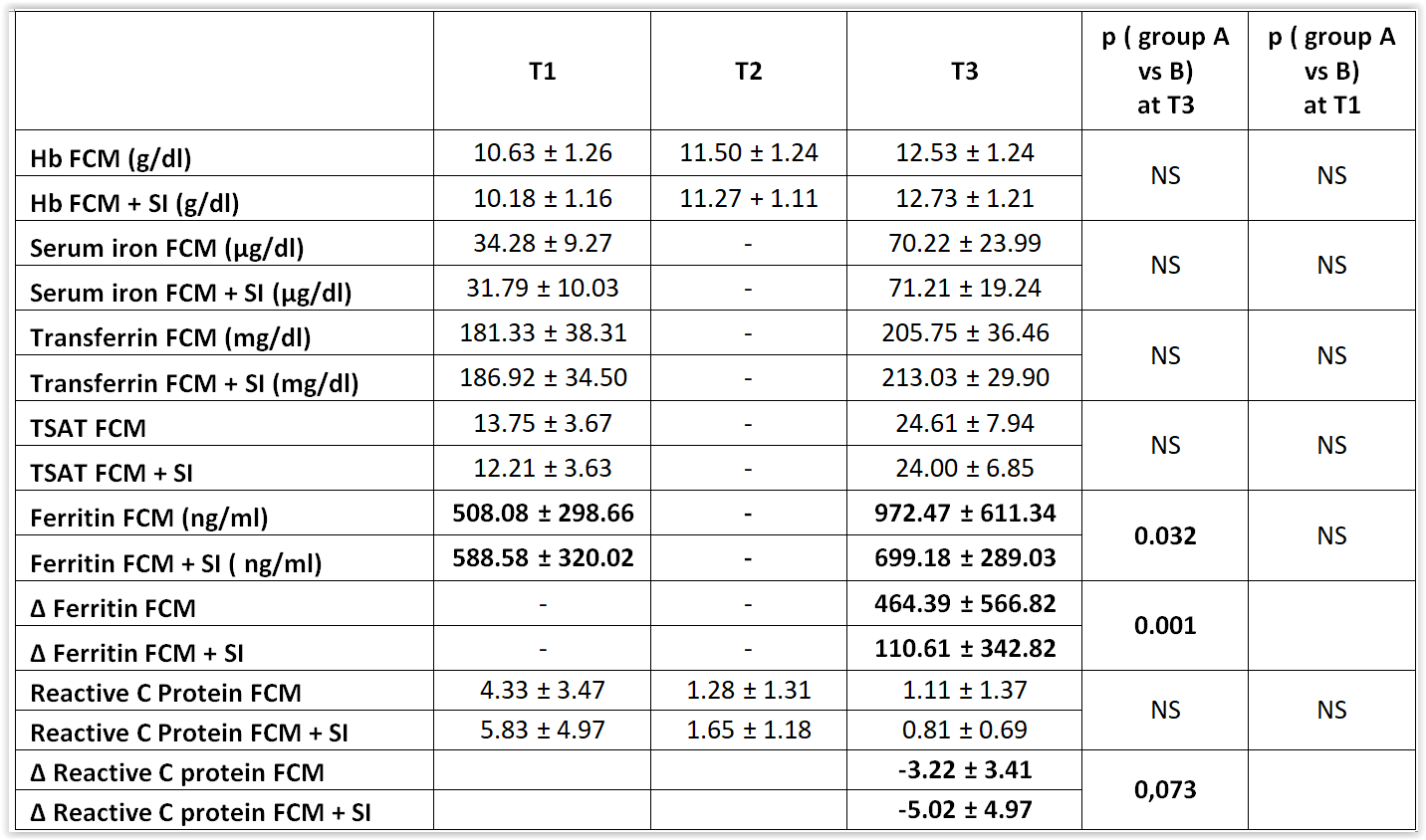
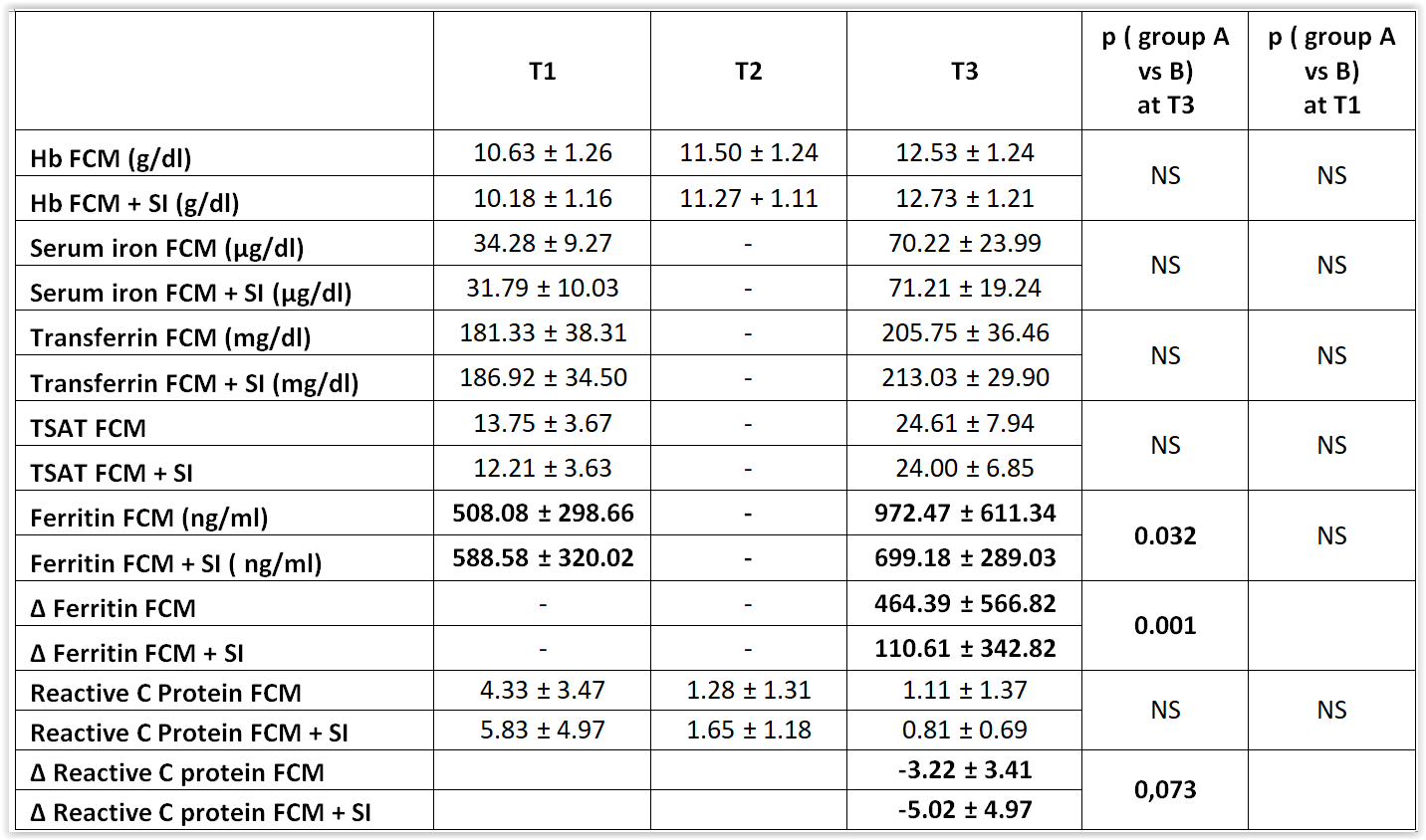
Background: Both carboxymaltose iron (FCM) and sucrosomial iron (SI) are effective in the treatment of iron deficiency anemia (IDA) after cardiac surgery (CS). However, intravenous iron, bypassing the reticuloendothelial system, may increase the risk of oxidative stress for the myocardium. The aim of this pilot study was to evaluate whether SI on top of FCM increases its efficacy on IDA, reducing the increase in ferritin (F), induced by FCM, and of C-reactive protein (CRP). Methods: 74 consecutive IDA patients (mean age 70.7 ± 9.1 years), admitted to Cardiac Rehabilitation after CS, were all treated with FCM (group A) and a part (group B, n 38) also with SI. The study design included a single dose of 1000 mg of FCM at T1 (8-10 days after CS) and in group B a dose of 60 mg of SI daily from T1 to T2 (the day of discharge 10 days later) until T3, 15 days later. Efficacy measures included changes from baseline in key hematological parameters (HP) and CRP. Results: Data are shown in Table. T HP increased significantly, with no difference between the two groups. However, Hb and transferrin saturation (TSAT) levels were lower at T1 in group B with a greater Δ increase [for Hb 2.5 and 1.9 (g/dl), for TSAT 11.8 and 10.8 (%) in FCM + SI group vs. FCM group, respectively]. Blood Iron was also higher in group B, although not significantly, starting from a lower baseline level. At T3 F levels were much higher in group A, almost doubling, despite being slightly lower at baseline (972.4±611.3 vs. 699.1±289 ng/ml; p. 032); Furthermore, ΔF was significantly higher (464.3 ± 566.8 vs. 110.6 ± 342.8 ng/ml; p.001). CRP decreased more at T3 in group B (although levels were higher at T1) with a greater ΔCRP (-5.0±4.9 vs. -3.2±3.4) approaching statistical significance (p.007). Conclusions: the high F levels are due to the inflammatory state induced by CS. The rapid increase in blood iron levels after intravenous administration, increases F in its turn and can activate macrophages through the release of cytokines and other inflammatory mediators. SI would seem to mitigate the increase in F and CRP, using the reticuloendothelial pathway and reducing oxidative stress and toxicity. Another positive effect of the combined therapy is the greater increase in Hb and TSAT which allows to reach the target for IDA more rapidly and to delay the subsequent administrations of FCM recommended by the Guidelines. A larger sample size may provide more meaningful results.