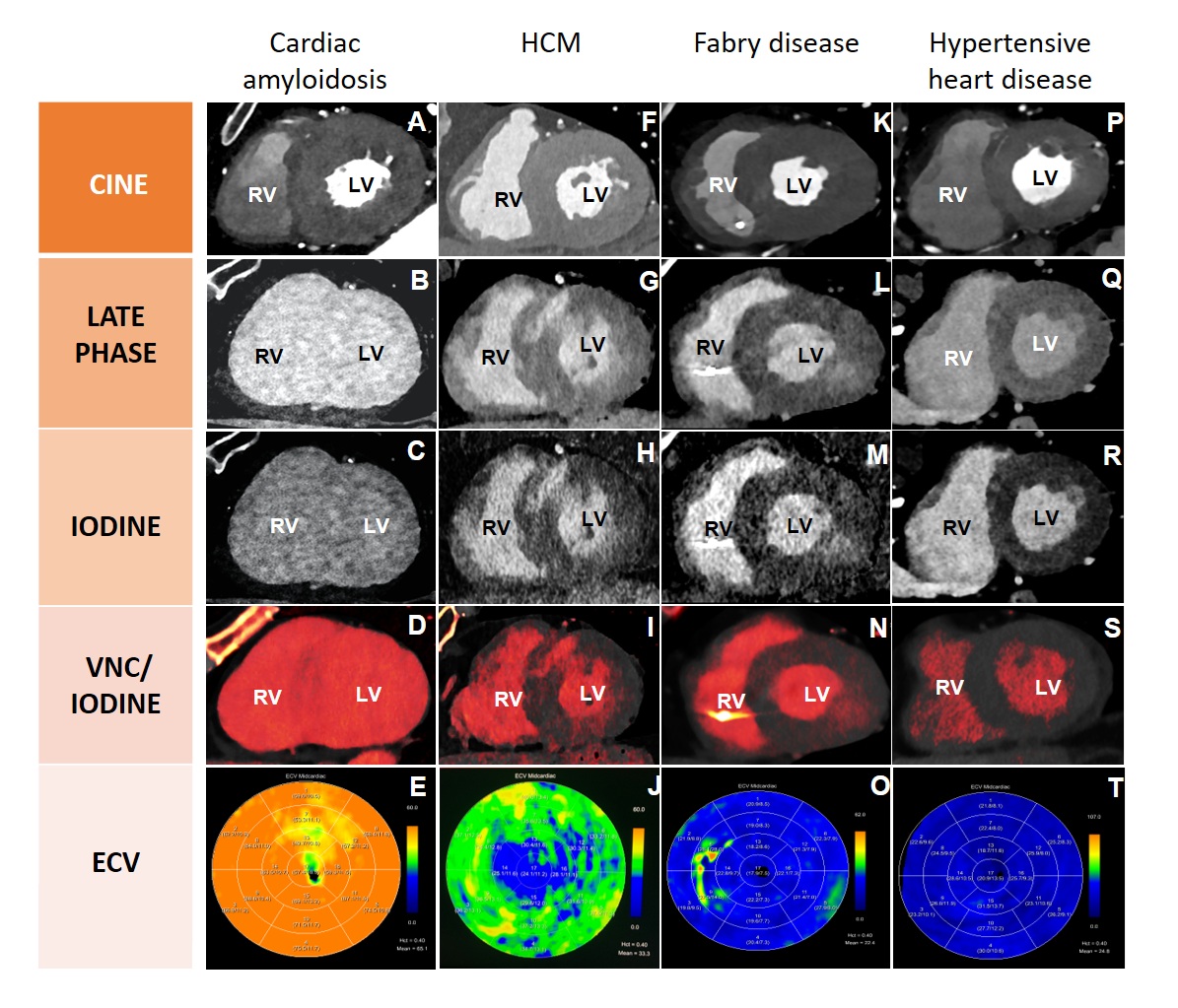
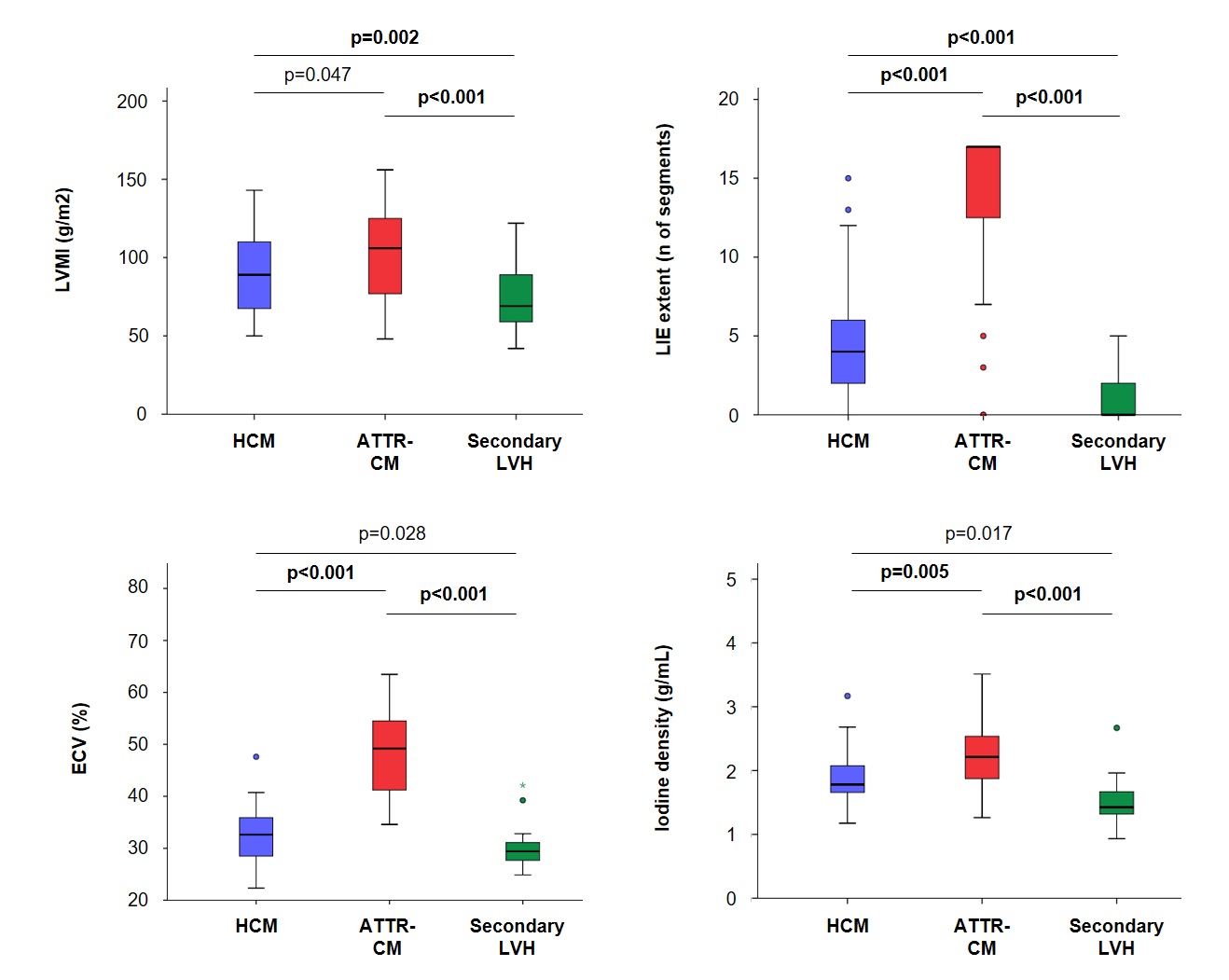
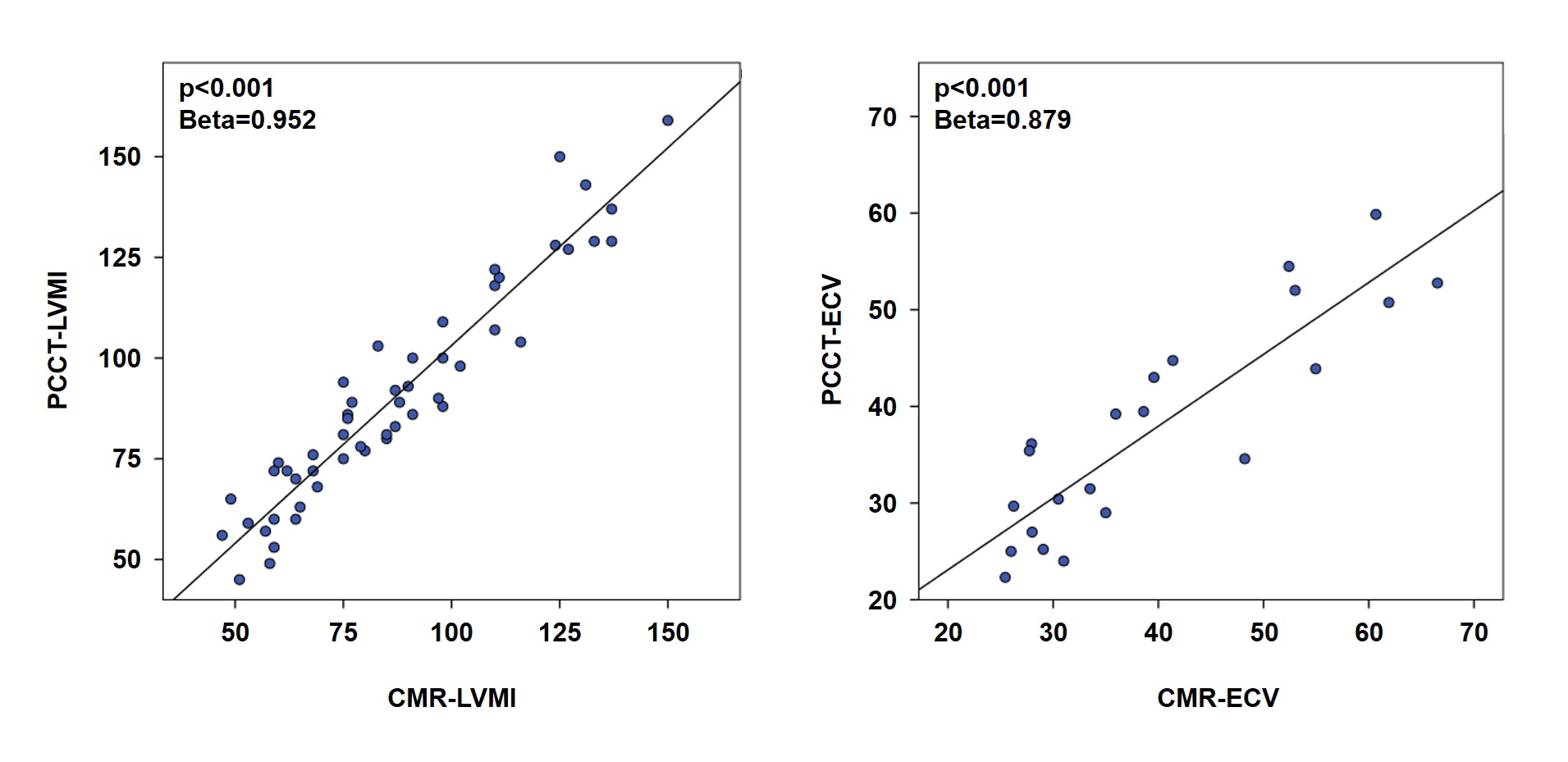
Background: Photon-counting computed tomography (PCCT) combines high spatial resolution with spectral imaging, and can thus provide a morphologic, functional and tissue assessment of hypertrophic hearts. We investigated whether PCCT can characterize left ventricular hypertrophy (LVH) as accurately as cardiac magnetic resonance (CMR) in the whole cohort and across hypertrophic phenotypes. Methods: Consecutive patients with LVH (n=123; 48 with hypertrophic cardiomyopathy [HCM], 36 with transthyretin cardiac amyloidosis (ATTR-CM) and 39 with secondary LVH) were referred to PCCT; 49 (40%) also underwent CMR within 12 months (median -31 days). Results: PCCT differentiated the three etiologies through distinctive tissue patterns. ATTR-CM showed the highest LV mass index (LVMI; median 105 g/m²), late iodine enhancement (LIE) extent (17 segments), extracellular volume (ECV; 45%) and iodine density (2.2 g/mL); secondary LVH displayed minimal fibrosis and the lowest ECV, while HCM had the greatest wall thickness but intermediate fibrosis burden. Morpho-functional indices from PCCT correlated closely with CMR (LVMI: beta=0.95, wall thickness: beta=0.98, LVEF: beta=0.91; all p<0.001). PCCT-ECV correlated with CMR-ECV in the overall cohort (beta=0.88, p<0.001), and segment-by-segment concordance for LIE versus late gadolinium enhancement was 98-100%. Iodine density correlated with CMR-ECV in ATTR-CM (beta=0.99, p=0.002) but not in HCM. Coronary assessment revealed ≥50% stenosis in 23%, and ≥70% in 10%. Conclusions: PCCT provides CMR-level accuracy for ventricular geometry, function and fibrosis while simultaneously visualizing coronary anatomy. Its ability to delineate distinctive tissue signatures (particularly the diffuse infiltration of ATTR-CM) suggests PCCT as an alternative when CMR is contraindicated or not available.