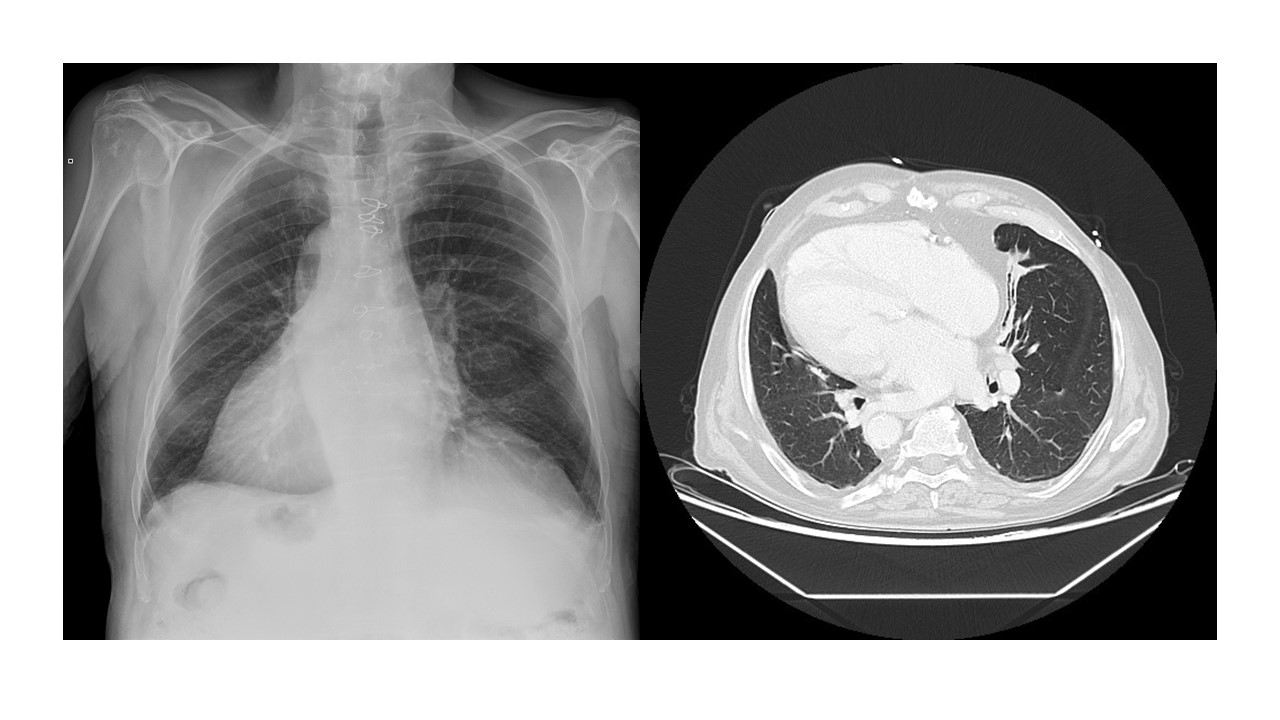
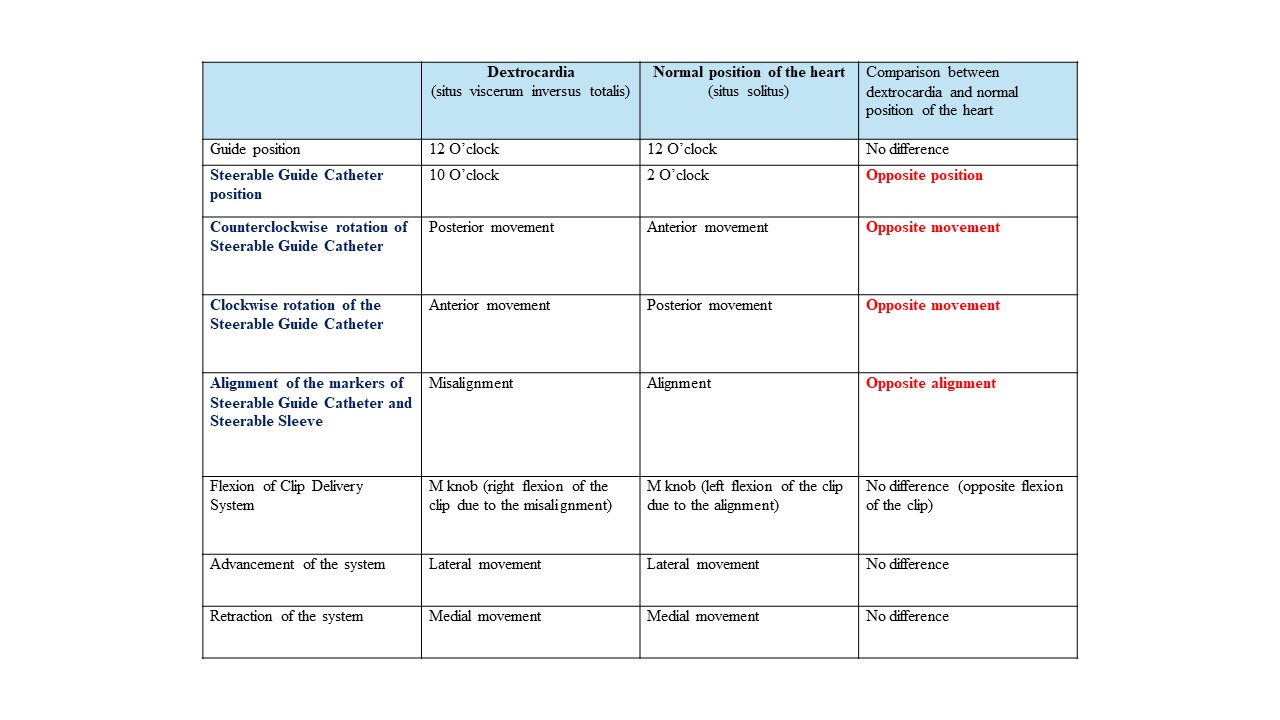
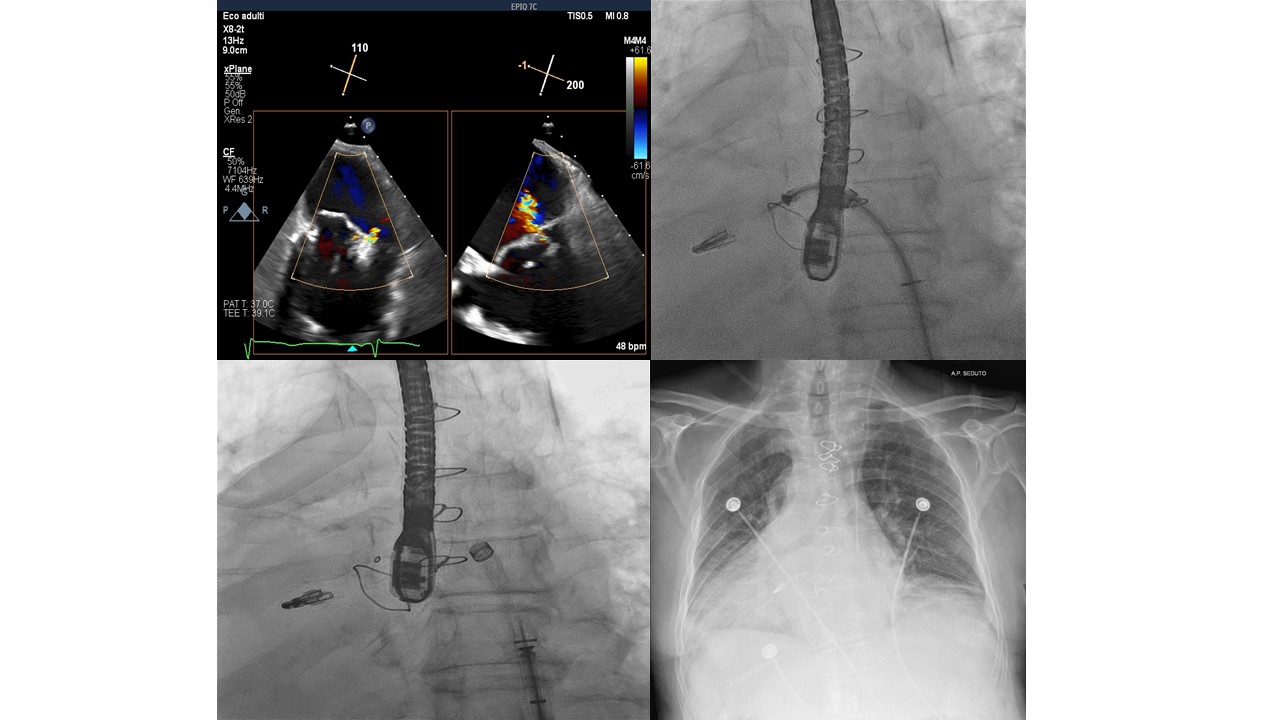
Case presentation. We reported an 86 years-old-man suffering from situs viscerum inversus totalis (Fig. 1), diabetes mellitus type 2, COPD, previous aortic valve replacement with Hancock 25 mm stented prosthesis and Vascutek 28 mm prosthesis for dissecting aneurysm of the ascending aorta. He was referred to our hospital for two episodes of heart failure (NYHA III). Transesophageal echocardiography (TEE) revealed severe mitral regurgitation (MR) due to flail of the anterior leaflet resulting in a central-lateral jet. Heart team determined that the patient was at high surgical risk for the treatment of mitral valve (MV); thus, we considered the MV transcatheter edge-to-edge repair (TEER) procedure using the MitraClip System. Pre procedural computed tomography did not reveal additional abnormalities. We gained access through the left femoral vein to have a straight access to the heart. The procedure was performed under fluoroscopy and TEE guidance. We punctured the mid-posterior part of the fossa ovalis, and advanced the tip of the steerable guide catheter (SGC) towards the right posterior side into the left atrium. The XTW clip was selected because of the length of the leaflets and the width of the mitral jet. We used an intentional 180° miskey of the clip delivery system when inserting into the SGC (misalignment of the markers on steerable sleeve and SGC), which led to the right flection of the clip using the M-knob to face of the MV (explanation in Fig. 2). We performed simultaneous grasping of both valve leaflets with immobilization of leaflets and reduction of regurgitant jet (Fig. 3) After the clip release, TEE showed the clip in stable position, residual MR grade I and mean pressure gradient 2 mmHg. At 6 months follow-up the patient was in functional class NYHA I and transthoracic echocardiography showed a stable result with persistence of MR grade I. Conclusion. An unusual anatomy can make the MitraClip procedure challenging, since the system guidance and steerability becomes more difficult, and imaging guidance is unpredictable. Mitral-TEER in a dextrocardia resulted in: 1) effective/persistent reduction of MR; 2) significant improvement in NYHA functional class/quality of life; 3) reduction in hospitalizations. The versatility of the MitraClip facilitated navigation of the system in this patient. Good planning of the procedure and collaboration between interventional cardiologist and echocardiographer are essential for procedural success.