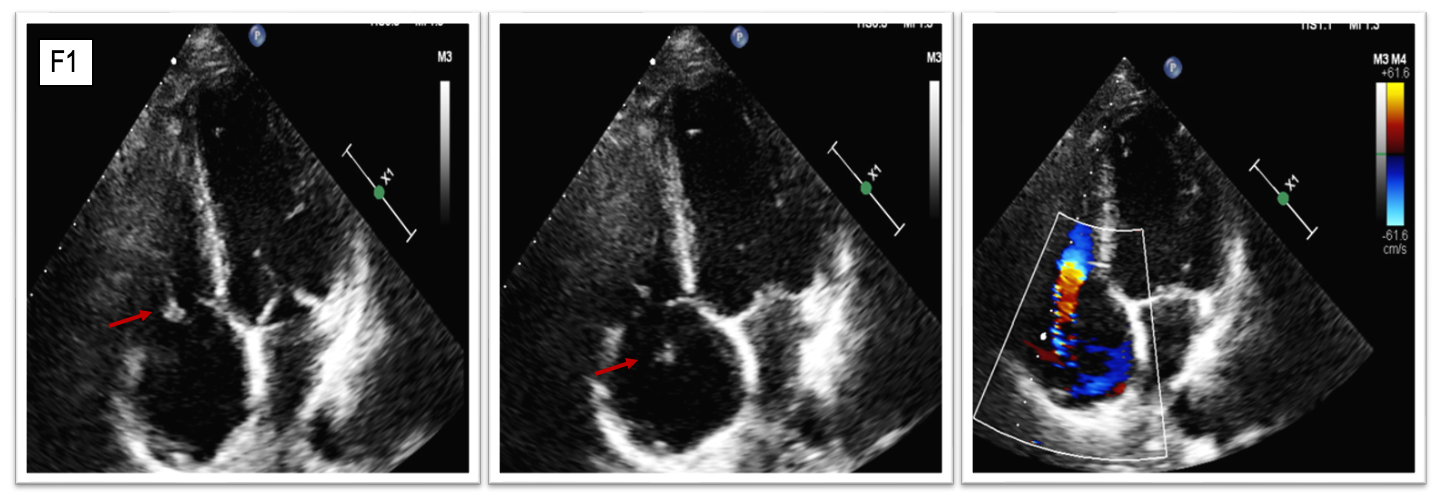
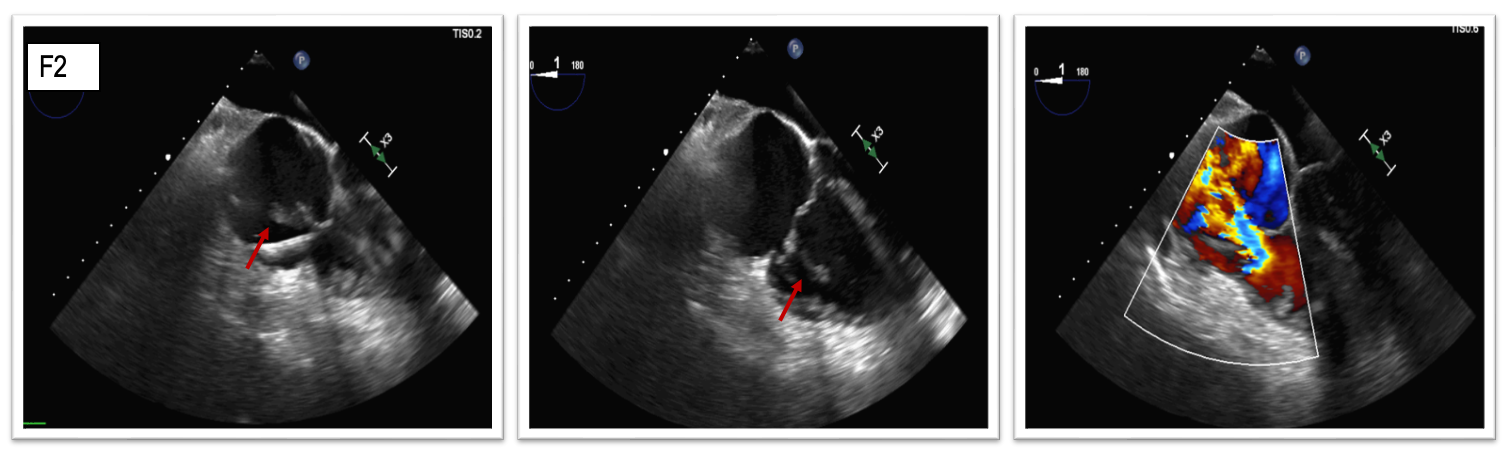
A 72 year old male presented to the emergency department with a two-week dyspnea, asthenia, and fever. His medical history included non-ischemic dilated cardiomyopathy, chronic kidney disease, previous left jugular vein thrombosis, COPD, and CRT-D implantation for primary prevention with recent re-implantation due to device pocket erosion. On admission, the patient was afebrile and showed signs of right-sided heart failure. Lab results indicated leukocytosis, elevated BNP, normal TnI, and persistently negative serial blood and urine cultures. Echo revealed a hypokinetic, dilated left ventricle (EF 30%), dilated right ventricle with normal function, moderate mitral regurgitation, VEXUS 3, and new-onset severe tricuspid regurgitation (VCW 8 mm, PISAr 9 mm) caused by septal leaflet flail with a mobile iso-echogenic lesion (Fig. 1). Transesophageal echocardiography revealed a filamentous, irregular and pedunculated structure attached to the septal leaflet of the tricuspid valve, projecting into the right atrium with a maximal dimension of 32 mm, initially suspected of endocarditis; leads were not involved (Fig. 2). High-dose intravenous loop diuretics and empirical broad-spectrum antibiotics were initiated without clear clinical benefits (NHYA III/IV). Thus, our main hypothesis became an iatrogenic papillary muscle rupture during lead extraction rather than an endocarditis. This was confirmed with PET/CT using 18F-FDG, which showed no hypermetabolic areas around the leads. After Heart Team discussion, we opted for TricValve implantation, given contraindications to surgery due to the patient’s high TRISCORE, poor clinical conditions and unfeasibility to transcatheter edge-to-edge repair due to the large coaptation gap with septal leaflet damage; percutaneous annuloplasty was also not indicated. Due to the presence of left brachiocephalic vein thrombosis limiting the superior vena cava implant, a single valve stent was successfully placed in the inferior vena cava via the right femoral vein (Fig. 3). Medical therapy was optimized, and after 6 months, there was no rehospitalization, signs of superior vena cava syndrome, with symptoms improvement (NHYA II). This case underscores the complexity of intracardiac device-related complications and the importance of a tailored intervention in patients with CIED related TR. A single valve stent might be an efficacy strategy to improve clinical symptoms in this scenario. Further studies on outcomes are needed.