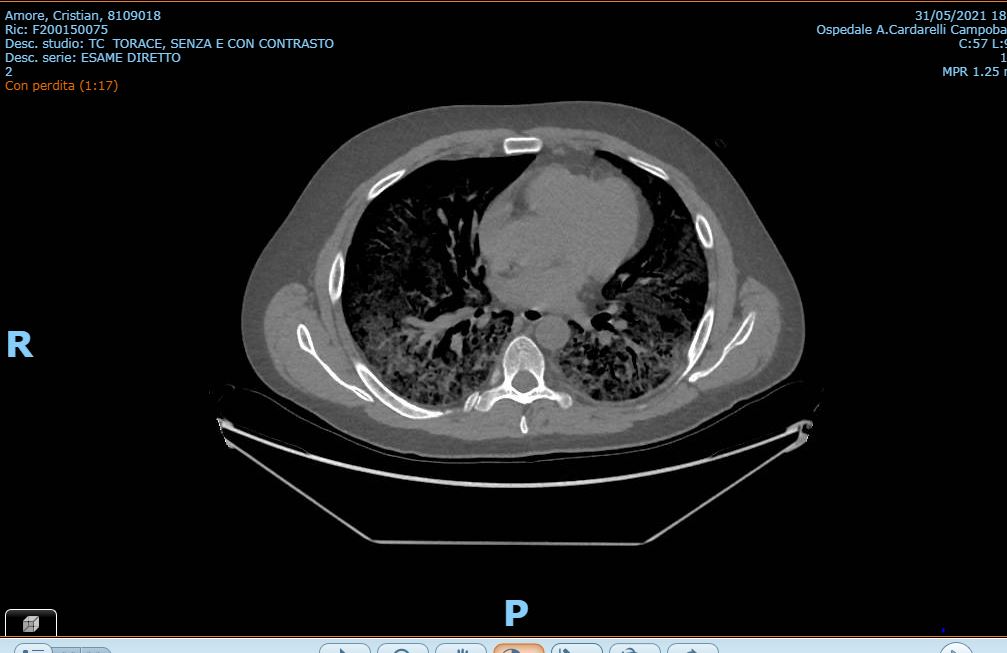
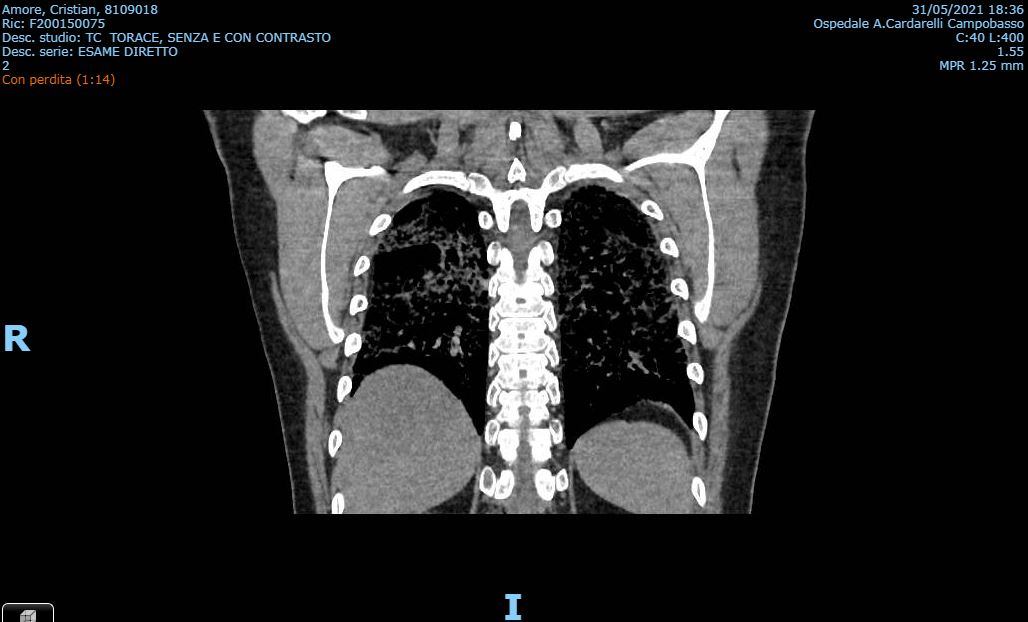
SARS-CoV2 is transmitted between humans via respiratory particles and the infection can presents with a large spectrum of manifestation. Prior studies have revealed a crucial role for cellular immunity in limiting the severity of the respiratory virus diseases. CD4+ T-helper are involved in several functions to coordinate and regulate antiviral immunity: they determine the development of high-affinity neutralizing antibodies and germinal centre B cell differentiation into memory and long-lived antibody secreting cells. No doubt about the crucial role played from T cell immunity response during SARS-CoV2 natural infection and after vaccination. We describe the case of a 39 old years man, who received the first dose of ChAdOx1-S vaccine. After two weeks he complained dyspnea and fever. SARS-CoV2 molecular test was negative; blood tests showed increased level of CPR. Chest CT excluded pulmonary embolism but revealed a bilateral ground-glass pattern suggestive for infection. Echocardiogram was performed showing normal findings. The ECG revealed only sinus tachycardia. The patient was discharged from the ED on corticosteroid therapy. A week later patient complained worsening of dyspnea. A new chest CT showed opacification defects in the secondary branches of lobar pulmonary artery and bilateral ground glass areas. LMWH and large spectrum antibiotic therapy was started. SARS-CoV2 molecular test and sierology was negative. Blood tests for Mycoplasma, Chlamydia, Legionella and CMV DNA test were negative. At the blood count lymphocytes levels were lower (6,8%) with a relative increased neutrophiles levels (90,4%) and normal WBC count. CT-HR showed a relevant bilateral crazy paving aspect, suggestive for a viral infection but also for a mycotic infection (the radiologist suggested a Pneumocystis Jiroveci Pneumonia pattern). HIV test had positive result; lymphocyte typing showed low levels of T-helper Lymphocytes (CD3+/CD4+) and a 0% of the CD4+/CD8+ ratio. The clinical condition worsened so that he was transferred to the ICU. After 30 days from the AIDS diagnosis the patient died. The role of T-lymphocytes in the development of high-affinity neutralizing antibodies and long-memory antibodies in SARS-CoV2 infection is the key of the vaccination strategy to reduce the spread of pandemic, but in our patient this mechanism failed and revealed the weakness of his T-Cell immune response due to HIV unknown infection.