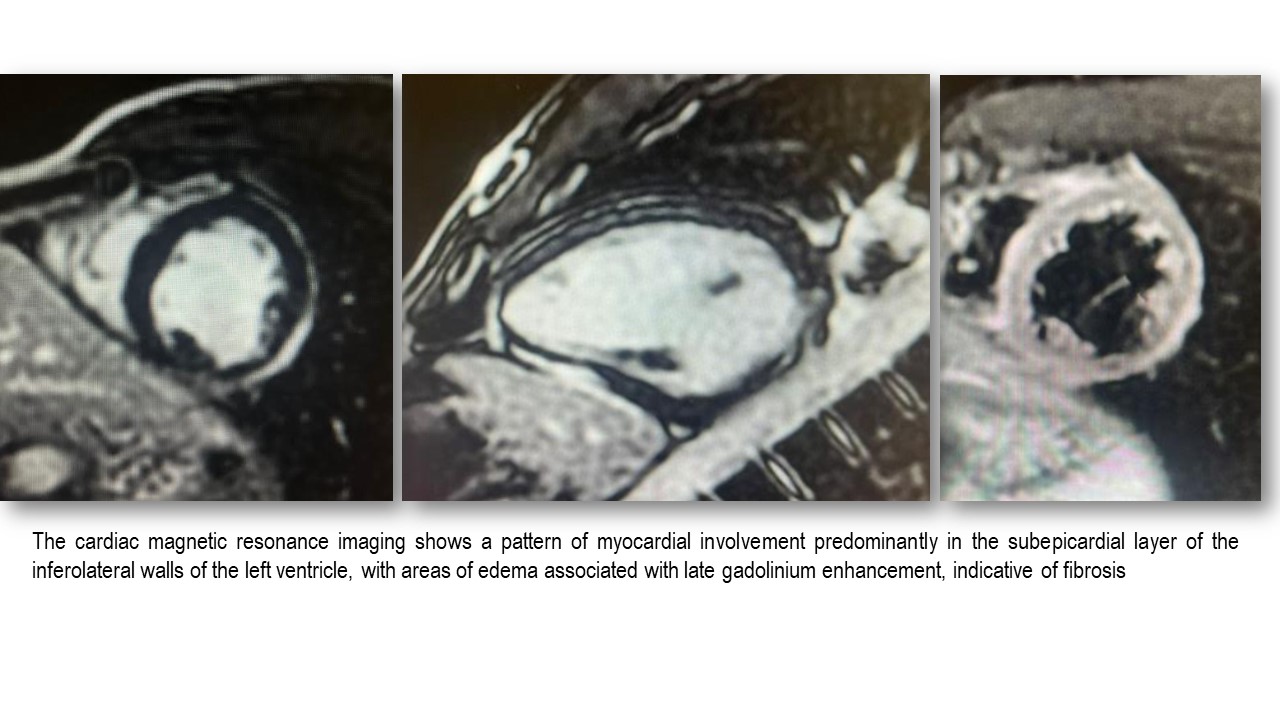
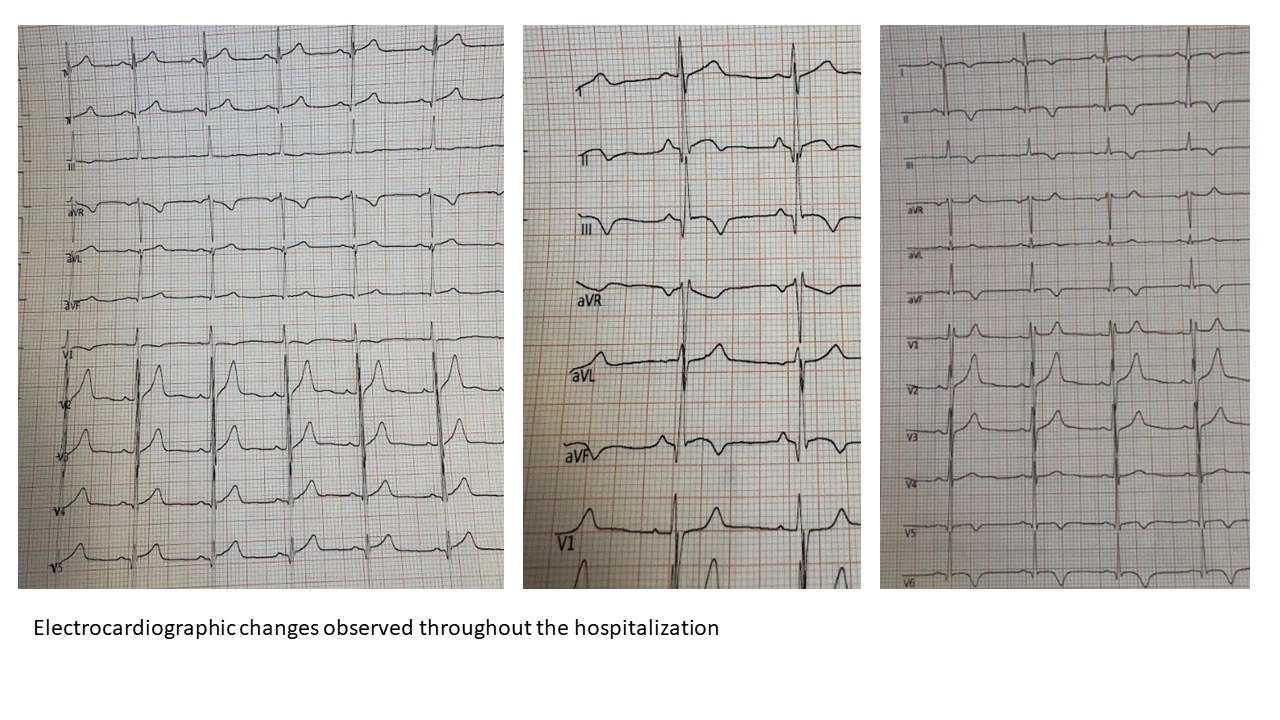
Introduction Becker muscular dystrophy (BMD) is an X-linked disorder caused by mutations in the dystrophin gene, characterized by progressive skeletal and cardiac muscle involvement. Cardiac involvement, often subclinical, affects up to 50% of patients and is typically characterized by myocardial fibrosis and fibro-fatty replacement of the inferolateral walls of the left ventricle. An acute presentation with features suggestive of myocarditis has been only rarely reported. Case We report the case of a 15-year-old male patient with BMD, without significant skeletal muscle involvement and with previously normal cardiac evaluations, who presented to the Emergency Department with acute chest pain. The initial electrocardiogram showed nonspecific repolarization abnormalities, while transthoracic echocardiography was unremarkable. Laboratory tests revealed a marked elevation of cardiac troponin levels (2476 ng/L; upper reference limit <14), in the absence of fever, elevated inflammatory markers, or recent infectious history. During hospitalization, electrocardiographic evolution was observed, characterized by ST-segment elevation in the inferior leads, development of Q waves, and deep T-wave inversion in the inferolateral leads. Echocardiography showed progressive hypokinesia progressing to akinesia of the infero-apical wall, associated with mild left ventricular systolic dysfunction (ejection fraction 53%). Cardiac magnetic resonance imaging demonstrated left ventricular systolic function at the lower limits of normal (ejection fraction 51%) and the presence of subepicardial late gadolinium enhancement in the inferolateral wall, consistent with a mixed pattern of myocardial edema and fibrosis. Treatment with an angiotensin-converting enzyme inhibitor, beta-blocker, and mineralocorticoid receptor antagonist was initiated, with progressive clinical, laboratory, and imaging improvement. Conclusions The absence of systemic inflammatory signs, identifiable infectious triggers, and the presence of pre-existing myocardial fibrosis make the diagnosis of classical acute myocarditis only partially plausible. This case suggests that, in patients with BMD, an acute presentation with chest pain and troponin elevation may represent a “hot phase” of dystrophin-related cardiomyopathy rather than true myocarditis. Recognition of this entity is crucial for accurate interpretation of cardiac magnetic resonance findings, therapeutic management, and long-term prognostic follow-up.