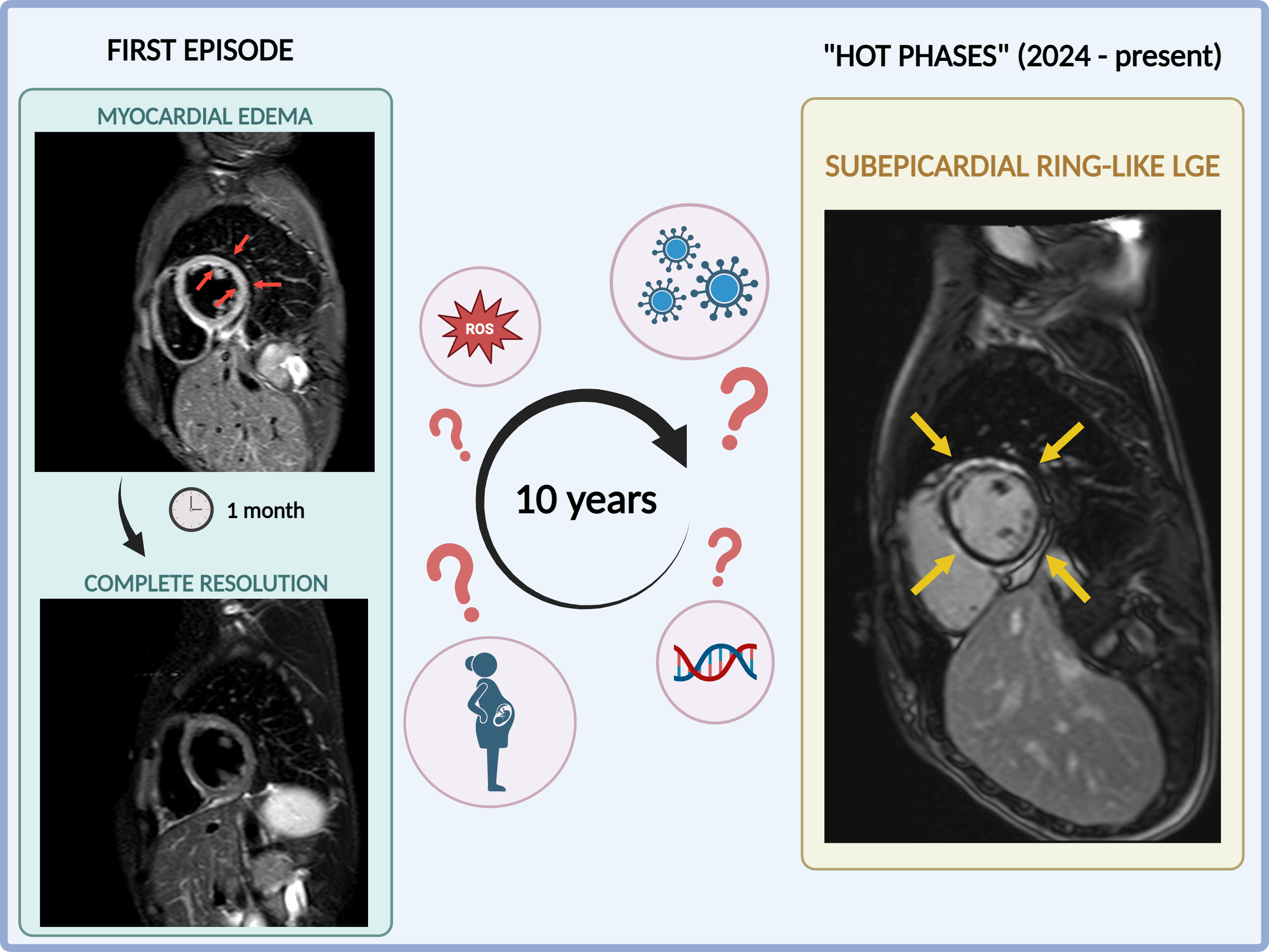
Arrhythmogenic Cardiomyopathy (ACM) is characterized by progressive fibrofatty replacement, predisposing to ventricular arrhythmias and sudden cardiac death. A distinct manifestation, particularly in Desmoplakin (DSP) mutation carriers, is the acute, inflammatory "hot phase," which can mimic myocarditis and accelerate structural remodelling. We report the case of a 28-year-old woman with a pathogenic DSP truncating variant. She had a history of presumed myocarditis (age 18, 2014) with initial Cardiac Magnetic Resonance (CMR) findings of transient edema and Late Gadolinium Enhancement (LGE) that were not suggestive of underlying cardiomyopathy and resolved completely upon subsequent follow-up. Two subsequent uncomplicated full-term pregnancies occurred over the next 10 years. In July 2024, she presented with recurrence (chest pain, elevated troponin, reduced Left Ventricular Ejection Fraction, LVEF 46%). Endomyocardial biopsy was non-specific (low infiltrate, viral/bacterial PCR negative). A follow-up CMR confirmed persistent biventricular myocardial fibrosis (subepicardial ring-like LV LGE, RV involvement). Over the following months, LVEF stabilized at approximately 40%; however, Holter monitoring documented 1,860 ventricular extrasystoles and non-sustained ventricular tachycardia. Genetic testing revealed a heterozygous truncating DSP pathogenic variant. Due to extensive fibrosis, progressive LVEF dysfunction and arrhythmia burden, an Implantable Cardioverter-Defibrillator (ICD) was recommended for primary prevention. She was re-admitted in September 2025 due to an exacerbation of myocardial injury. A repeat CMR demonstrated stability of the LGE pattern, confirming biventricular involvement but crucially, the absence of edema. Consequently, ICD implantation was planned and recently performed. The proband's father presented with atrial fibrillation (AF) and a LVEF of 35% in 2024. Despite initial suspicion of tachycardia-induced cardiomyopathy and failed AF ablations, a post-procedure sinus node dysfunction and the established family history of ACM led to the indication for ICD implantation during the same hospitalization. This case underscores the distinct inflammation-driven nature of ACM secondary to a DSP variant, characterized by recurrent "hot phases," rapid LVEF decline, and extensive biventricular fibrosis. Genetic confirmation enabled accurate risk stratification and timely primary prevention ICD implantation in two affected family members.