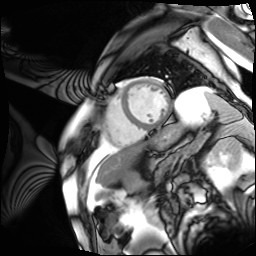
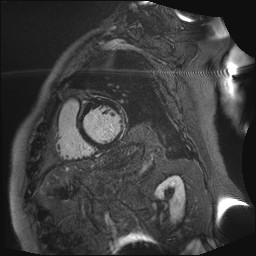
A 71-year-old patient with a history of atrial fibrillation (AF), under treatment with flecainide, apixaban and metoprolol, was admitted to the emergency department presenting with dizziness. There was no family history of heart disease. The initial electrocardiogram (ECG) revealed a wide QRS complex tachycardia with a right bundle branch block (RBBB) morphology, lasting a few minutes, which responded promptly to intravenous amiodarone, prompting the discontinuation of flecainide. The patient remained hemodynamically stable throughout. He was admitted to the cardiology unit for further evaluation. The baseline ECG showed atrial flutter. Transthoracic echocardiography showed mild left ventricular dysfunction without other significant abnormalities. Coronary angiography ruled out significant epicardial coronary artery disease. Continuous electrocardiographic monitoring showed evidence of atrial flutter with variable conduction. Therefore, after excluding left atrial appendage thrombus via transesophageal echocardiography, successful electrical cardioversion was performed. Due to persistent mild LV dysfunction, cardiac magnetic resonance imaging (CMRI) was scheduled. T1-weighted sequences demostrated extensive subepicardial fat infiltration affecting the infero-lateral and antero-lateral walls of the left ventricle. Late gadolinium enhancement (LGE) revealed widespread subepicardial enhancement in the same regions, partially extending to the mid-inferior and anterior segments, producing a ring-like pattern. The right ventricle appeared structurally normal. Although no universally accepted criteria currently exists for diagnosing ALVC, the recent European Task Force consensus report, support a diagnosis of ALVC. The initial arrhythmia was interpreted as a sustained monomorphic ventricular tachycardia with RBBB morphology, a hallmark feature of ALVC. Consequently, an implantable cardioverter-defibrillator (ICD) was placed for secondary prevention.